Chapter Four
FINDINGS
4.1. SOCIO-DEMOGRAPHIC CHARACTERISTICS OF RESPONDENTS
INVOLVED IN
THE SURVEY
One hundred fifty (150) respondents were interviewed in the
survey, of who 81 (54%) were from Kintampo Sub-District, 41(27%) from Jema
Health Sub-District and 28 (19%) from New Longoro Sub-District. Majority (71%)
were from urbanized settlements.
In total 65 individuals of different socio-demographic
background, 29 (45%) females and 36 (55%) males were part of key informant
participants in the qualitative study, with ages ranging from 20 to 64 years
and a mean age of 30.6 years (SD 11.78). Seventeen of them (26%) ,made up of
the District HIV-AIDS response initiative coordinator, the District Public
Health Nurse in Charge of Family Health Clinic, the different religious
leaders, one traditional herbalist, one laboratory technician, one medical
doctor, 3 newly married couples (old couples), one prospective would-be couple,
one single influential young boy and one counselor, were key informants
contacted for In-Depth Interview (IDI) whereas the majority (74%), made up of
unmarried young adults and parents, took part in Focus Group Discussions.
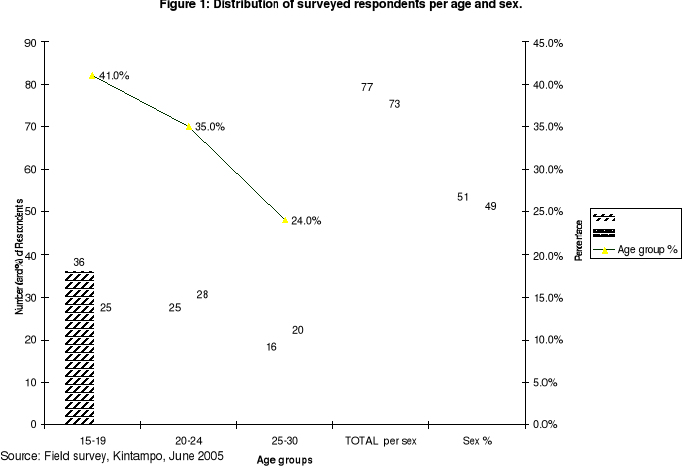
4.1.13.
DISTRIBUTION OF RESPONDENTS BY AGE AND SEX
The 150 surveyed respondents were unmarried young adults aged
between 15 and 30 years with a mean age of 21.0 years (SD 4.48), the majority
of them (76%) being aged between 15-24 years (age distribution left skewed).
The sex distribution of respondents was slightly skewed with a little but
insignificant predominance of males (51%) [p-value=0.29]. Figure 1 below
describes these features.
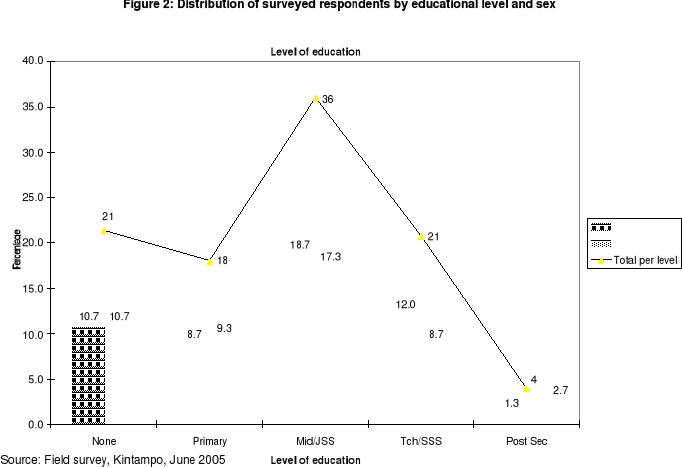
4.1.2. EDUCATIONAL BACKGROUND OF
RESPONDENTS
The educational features of respondents in the survey (Figure
2) ranged from those with no formal education to post secondary school level,
majority of them (36%) being in Middle continuation and Junior Secondary
Schools (JSS), constituting a quasi-normal distribution. In both sexes the
trend showed an increased number from primary school level to Middle/JSS level
followed by a progressive sharp decrease of respondents in the subsequent
higher levels up to Post Secondary School, with no respondent at University
level at all. The trend also showed many surveyed males predominated over
females in Middle/JSS and Senior Secondary Schools (SSS) whereas surveyed
females were predominant in Primary and Post secondary schools (Figure 2). The
average number of years successfully completed at the highest level reached by
respondents was 3.
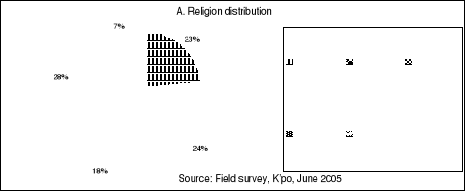
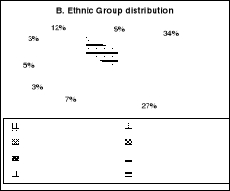
4.1.3. RELIGION, ETHNIC GROUP AND
OCCUPATION BACKGROUND
Majority of responds were mostly Christians (65%), followed by
Moslem (28%), the minority (7%) being without any defined religion.
Almost half part of respondents belonged to Akan (34%) and Mo
(27%) ethnic groups.
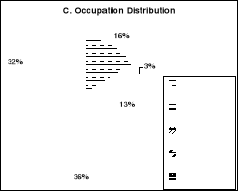
A higher proportion of respondents were students (36%),
followed by farmers (16%), with a minority of government or salaried workers
(3%).
All these features are summarized in Figure 3 below.
Figure 3: Distribution of Respondents by Religion, Ethnic
group and Occupation.
4.2. PREMARITAL SEX HISTORY AND HIV-AIDS RISK FACTORS
AMONG SURVEYED RESPONDENTS
Out of 150 respondents, 99(66%) have had premarital sex
already (78% of females and 55% of males), majority involved being females
(58%). Results in Table 3 show that female respondents were 2.97 times more
engaged in premarital sex than males (p-value =0.004116).
|
Table 3: Distribution of respondents according to
premarital sex history and sex.
|
|
Have had sex
|
Statistics (CI 95%, p<0.05)
|
|
Sex
|
Yes
|
No
|
Total
|
OR:2.97 (1.38<OR<6.46)
|
|
Female
|
57 (78%)
|
16 (22%)
|
73(100%)
|
RR: 1.43 (1.13<RR<1.82)
|
|
Male
|
42 (55%)
|
35 (45%)
|
77 (100 %)
|
X2 (Yates): 8.23
|
|
Total
|
99 (66%)
|
51 (34%)
|
150 (100%)
|
p-value: 0.004116
|
|
Source: Field survey, Kintampo, June 2005
|
Respondents in FGD mentioned the following as being the major
contributory factors to premarital sex in Kintampo District:
|
- The fact that Kintampo is highway stop over where over
night girls sell their goods to passengers,
- Curiosity, Peer pressure
- Type of songs and dances broadcast
- Lack of sex education in families,
- Bad dressings (mini skirts, tight clothes, half-naked
clothes): e.g.«Apuskelenke»
- Pornographic films, drug abuse, alcohol
- Unfaithfulness between married couples
|
- Poor parental care,
- Broken homes/marriages,
- Financial problem (poverty),
- Illiteracy and lack of education
- Joblessness, streetism, prostitution
- Modernism which breaks some protective traditional
social norms
- The human nature calling for satisfaction of sexual
physiological need,
- Single parents, - Traveling alone...
|
|
(Source: Compilation from IDIs and FGDs, Our Research
work, Kintampo, June 2005)
|
The age at first sex ranged from a minimum of 10 years up to
a maximum of 25 years and for the whole sample the mean age at first sex was
18 years (SD:2.98). However the mean age at first sex was 18.125 years (SD:2.6)
for females and 18.075 years (SD:3.34) for males, meaning both male and female
respondents engaged in premarital sex at about same age of 18 years . The
earliest age at first sex was 10 years in males and 12 years in females, the
latest age at first sex being 25 years in both sexes. Also the trend showed a
gradual increase of first sex rate as the age increases, the peak age of first
sex being 20 years in males and 18 years in females. Figure 4 describes these
features.
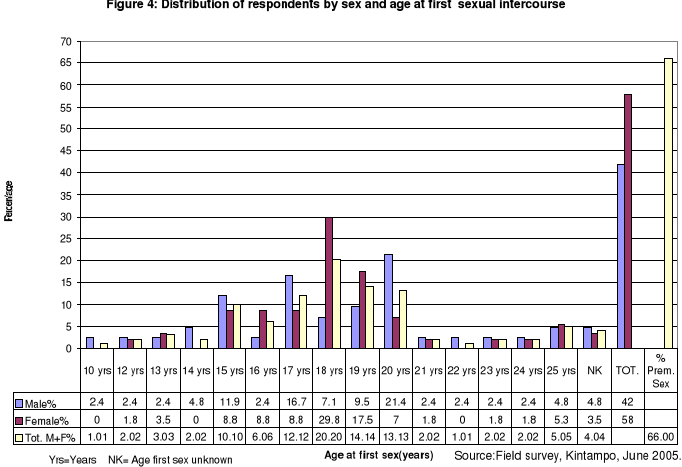
In addition, the number of sexual partners among those who
have had sex ranged from 1 to 15, with a mean of 2.7 (SD:2.38) partners per
respondents.
These findings reinforce trends from qualitative study where
participants attested to the fact that premarital sex was normal in Kintampo
society. This notion is captured in the responses below during IDIs and
FGDs.
|
«There is stage of age that when you reach, something
pushes you into it. And especially these days, the younger girls are very neat
and when you see them, they attract you and you just find yourself
psychologically attracted, so the next steps can follow....»
(FGD: A young boy during a mix boys-girls Christian FGD,
18 years old).
|
|
«In our times, children and young adults were supposed to
be home at 6:00 PM and slept not later than 8:00 PM. This helped us to be free
from premarital sex and its consequences such as STI/HIV-AIDS. But theses days,
if you go round to night in the streets, you find most of children and
adolescents, especially girls still wandering outside, pretending selling goods
while selling rather their bodies. They even commonly say: 'Sex for CFA',
meaning you have CFA or foreigner currency, you have me.»
(IDI: Rev Pastor, Pentecostal Church, Kintampo)
|
|
«Whatever the case, premarital sex cannot just be
eliminated; it is difficult to prevent it. Young boys and girls think it is a
spiritual disease. They said there is stages when you reach you feel like
having sex. And for that matter the best we could do is just to tell them they
should use condom. If you ask them to abstain, you are
lying.»
(FGD: A 54 - year-old traditionalist
father, parent FGD /Ampoma)
|
|
«The fact of Kintampo being in the Middle way from
North to South Ghana is bringing us troubles. Sex workers and young girls
because of stopover all over days and nights feel comfortable in their sex
business. They don't even use condom to protect themselves. All they want is
money. Because men say raw sex is the sweetest, they pay higher fees for it.
The fees are different depending on who the client is. A Ghanaian is asked to
pay 50,000 Cedis, whereas foreigners pay 150CFA per sexual greetings. So
premarital sex in Kintampo has become part of the natural life here. So
HIV/AIDS is part of our every day stuffs. If the situation is to be solved,
then may be the government should make a policy which prohibit all stopovers
here and all sorts of trade overnight. Girls and boys found in the street
overnight should be arrested by the police...»
(One young girl,24years old, KHRC field worker during a
female Moslem FGD in picture No 1)
|
|
|
«In my opinion, I think it is wise to test for
HIV/AIDS before one marries. This is because one may not know the past life of
the fellow fiancé(e).In this modern times, marriages are no longer done
holily due to the fact that most would-be couples might have engaged in
premarital sex that expose to all kind of risks. So since I am not sure
premarital sex in younger adults could be totally eradicated in this spoiled
town, I fully support the view for HIV premarital counseling and testing,
another alternative to fight HIV/AIDS.»
(IDI: A young Christian boy, 25 years old, in Picture No
2)
|
4.3. GENERAL AWARENESS AND KNOWLEDGE OF RESPONDENTS ON
HIV/AIDS,
VCT AND HIV PCT
|
Table 4: Trend of general awareness and knowledge on
HIV/AIDS, VCT and HIV PCT
[Chi-Square, Note: X2(Y)=Yates corrected
chi-square, p<0.05, CI:95%]
|
|
Indicators on awareness and knowledge on HIV/AIDS,
VCT and HIV PCT
|
Yes (%)
Male
(N=77)
|
Yes (%)
Female
(N=73)
|
Yes (%)
Total
(N=150)
|
p-value
X2*
OR
|
|
1.Knows or have known a young adult who suffers/suffered from
HIV AIDS
|
32(41.6)
|
31(42.5)
|
63(42.0)
|
OR=0.96
p=0.95
|
|
2. Know that unprotected pre-marital sex with casual/multiple
partners is a risky behaviour that could expose to STI-HIV/AIDS
|
74(96.1)
|
71(97.1)
|
145(96.7)
|
X2=1.95
p=0.375
|
|
3. Know that a child could be born HIV positive from sexual
union of his/her parents/mother
|
70(90.9)
|
66(90.4)
|
136(90.7)
|
X2=5.6
p=0.0604
|
|
4. Know that HIV/AIDS does not have any effective cure yet
|
71(92.2)
|
71(97.3)
|
142(94.7)
|
OR=0.33,
p=0.31
|
|
5. Know that not all sexual unions and marriages are safe and
good for health of both partners and offspring:
|
47(61.0)
|
45(61.6)
|
92(61.3)
|
X2=3.39
p=0.1833
|
|
5.1.Know that HIV/AIDS makes unsafe sexual unions
and marriages
|
33(42.9)
|
26(35.6)
|
59(39.3)
|
X2=1.15
p=0.7664
|
|
5.2. Know that others diseases a part from HIV/AIDS
makes
unsafe some sexual unions and marriages
|
7(9.1)
|
7(9.6)
|
14(9.3)
|
|
5.3. Know that both HIV/AIDS and others diseases make
unsafe sexual unions and marriage
|
9(11.7)
|
12(16.4)
|
21(14)
|
|
6. Recognize that they will consider health status as core
criteria when they choose their marriage partners
|
74(96.1)
|
68(93.2)
|
142(94.7)
|
OR=1.8
X2(Y)=0.19
|
|
7. Way to assess «Good Health Status» of marriage
partner before marriage: 7.1.By observing his/her appearance
|
3(3.9)
|
4(5.5)
|
7(4.7)
|
-
|
|
7.2.By asking close family
member
/friends
|
5(6.5)
|
5(6.8)
|
10(6.7)
|
|
7.3.Through premarital
medical
examination
|
66(85.7)
|
58(79.5)
|
124(82.7)
|
|
8. Have ever heard about HIV voluntary counseling and testing
(VCT)
|
53(68.8)
|
55(75.3)
|
108(72)
|
OR=0.7, p=0.48
|
|
9. Have ever heard about HIV premarital counseling and
testing
|
62(80.5)
|
65(89)
|
127(84.7)
|
OR=0.5, p=0.22
|
|
10. Sources of information about HIV PCT :
10.1.Radio/TV/Cinema/Video
|
61(83.5)
|
52(73.2)
|
113(78.5)
|
-
|
|
10.2. Churches or
mosques
|
22(30.1)
|
30(42.2)
|
52(36.1)
|
|
10.3.Friends/third
person
|
15(20.5)
|
32(45)
|
47(33)
|
|
10.4. Health workers
|
26(35.6)
|
20(28.2)
|
46(31.9)
|
|
10.5.Schools/University
|
23(31.5)
|
18(25.3)
|
42(29.2)
|
|
10.6.News papers or
books or posters
|
16(22)
|
11(15.5)
|
27(19.75)
|
|
10.7 .Parents
|
10(17)
|
10(14)
|
20(14)
|
|
10.8.Conference/youth
camp
|
5(6.8)
|
2(2.8)
|
7(4.9)
|
|
10.9. Internet
|
2(2.7)
|
3(4.2)
|
5(3.5)
|
|
10.10. Others sources
|
1(1.36)
|
1(1.4)
|
2(1,38)
|
|
11. Know that HIV PCT is one of the main measures to limit the
spread of HIV/AIDS in new couples
|
70(91)
|
68(93)
|
138(92)
|
X2=1.01
p=0.6
|
|
12. Know of someone or a couple who underwent HIV PCT before
marriage
|
26(34)
|
29(40)
|
55(37)
|
X2(Y)= .35
p=0.55, OR=0.7
|
|
13. Knowledge of who is required to undergo Premarital
Counseling and Testing (PCT): 13.1.The male partner
|
11(14.3)
|
2(2.7)
|
13(8.7)
|
-
|
|
13.2.The female partner
|
1(1.3)
|
8(11)
|
9(6)
|
|
13.3.Both partners
|
65(84.4)
|
63(86.3)
|
128(85.3)
|
|
14. Know major advantages of HIV PCT:
|
|
|
|
-
|
|
14.1.To know about their health and HIV status so
that
they decide responsibly about
marriage
|
67(87)
|
61(83.5)
|
128(85.3)
|
|
14.2.Stability and safety in marriage
|
36(47)
|
32(44)
|
68(45)
|
|
14.3.It strengthens marital relationship and
enhance
marriage satisfaction
|
23(30)
|
20(27.4)
|
43(29)
|
|
14.4.To ensure fertility in couples
|
17(22)
|
14(19)
|
21(14)
|
|
Source: Field survey, Kintampo, June 2005
|
In general, the main trend of awareness and knowledge of
respondents on HIV/AIDS, VCT and HIV PCT summarized in Table 4 are the
following:
Less than half of respondents of both sexes knew of any young
adult who suffer/suffered from or died of HIV/AIDS, male respondents knowing
less than females, but with no statistical significant difference between both
sexes.
|
«Yes, HIV/AIDS is common here. When you get
it you will not die early. My own 18 years old Junior Uncle had it. He would
grow thin and later grow big, grow thin and grow big again, and long round he
finally grew thin, became so sickly and died. He might have left the insect to
his girl friends, so those who will later marry them will come across deadly
spouses. I am afraid of this.»
(IDI: A 57-year-old Traditional herbalist/Ampoma,
father of 5 children, Picture No 3).
|
|
More than 96% of both males and females respondents knew
unprotected premarital sex with casual and multiple partners expose to
HIV/AIDS, no statistical significant difference between them.
Also more than 90% of both males and females knew that HIV
could be transmitted from mother to child through sexual union of parents,
again the trend shows no statistical significant difference between the two
categories.
|
«HIV/AIDS is a big curse. Children and generations
can all become infected and affected by it from their parents. It brings
problems to the family and the whole nation. So many widows and widowers, so
many orphans, so many deaths. No longer happiness in family at all. So if this
could be prevented by like HIV Premarital check-up for current younger people,
it is better.»
(A 32-year-old female parent: FGD of Moslem
mothers)
|
94.7% of respondents were aware that HIV/AIDS does not have
any cure yet (no statistical difference between both sexes). This finding is
obvious since in Kintampo society even some traditional healers are aware of
this fact. They are currently taking advantage of the inexistence of any
effective cure against HIV/AIDS to attract the community members to their
services, pretending they have traditional drug to cure HIV/AIDS (See
illustrative pictures below):
Pictures 4 and 5: Poster of an herbalist on the main road just
at Apaaso, Kintampo Police barrier
Source: Our Research Inquiry on
the field, Pictures No 4 and 5.
Majority (>60%) of both male and female respondents were
similarly aware that not all sexual unions and marriages are safe and good for
health of both partners, and their offspring ( no statistical significant
difference). However, surprisingly fewer (42.9% of males and 35.6% of females)
knew that HIV/AIDS makes unsafe sexual union and marriage.
|
«We all know not all sexual unions and marriages are
healthy for spouses and their children. Many diseases can bring problems and
instability in the family. So sometimes we consider all these before giving our
children to somebody for marriage»
(A 30-year-old young parent, FGD of Traditionalist
fathers/Ampoma)
|
A higher number of both males (96.1%) and females (93.2%) were
similarly aware that they will consider health status as core criteria when
they will choose their marriage partners.
In all FGD and IDI, all participants also strongly considered
health status is the major criteria in choosing spouses.
|
«Well. No body wants to die or to kill
him(her)self. Because when you see that your prospective spouse is having the
disease like HIV, obviously you go away from him/her to protect your self. This
is the least natural auto defense a normal human being could
do».
(A 26-year-old mother, FGD of Traditionalist
mothers)
|
|
«Do not take your self to where you will perish or
where you will endanger others. If you do, it is equivalent to committing
suicide or homicide. The prophet said you should not cheat and somebody should
not also cheat you...The prophet talked about `examine a woman very well before
taking her into marriage...Because it is from this examination you will be able
to tell whether you should go ahead or stop the marriage process'. It is a
matter of life or death. Anything you see that could shorten your life and even
the marriage is significant. Nothing is as dangerous as HIV/AIDS
today».
(IDI: The Imam, Kintampo Central Mosque, Picture No
6)
|
|
Although the neat majority of males (85.7%) and of females
(79.5%) recognized premarital medical examination as the right way to assess
«Good health status» of their marriage partners, a few part of them
thought they would assess it simply by observation of external appearance
(4.7%) or by asking close family members (6.7%). There was no significant
statistical difference between the trends in both sexes.
In all FGDs and IDIs all participants said premarital medical
examination was not included in the marriage procedures in Kintampo and showed
a great disagreement to this sort of managing marriage, saying PCT was very
important.
|
«No! In the older times it was good not to
conduct premarital examination, but these days it is not good to skip it. In
the past-time there was no premarital sex epidemic like today. There were no
doctors, no tests nor laws to encourage premarital examination. But still there
were rudimentary ways to study good health status of a person to marry. So
nowadays medical examination must be a law in our society and
churches.»
(A 45-year-old Christian father: FGD of Christian
parents, Picture No 7).
|
|
|
«At first we weren't aware of premarital examination
in our Islamic religion. But now we have realized that it should be done
before marriage since some diseases are hidden»
(A 22-year-old mother: FGD of Moslem mothers/Kintampo
central mosque, Picture No 8).
|
|
«I may trust my child and if someone comes to marry
her, I have to see it that premarital examination is done, before I accept the
marriage go ahead»
(A 46-year- old mother: FGD of Traditionalists
mothers/Ampoma).
|
Surprisingly, although HIV PCT is a specific type of VCT,
majority of respondents (84.7%) had heard more about HIV PCT than VCT itself
(72%). No significant statistical difference in males and females trends.
The top source of information on HIV PCT among respondents was
through Radio, TV, Cinema or Video (78.5%), the second source being churches
and mosques (36.1%), followed by friends or third person (33%). Worst still
parents were at the seventh position (14%).
In both sexes, HIV PCT was well known as one of the major
measures to limit the spread of HIV/AIDS in new couples. No statistical
difference between the trends in the 2 groups.
|
«Premarital examination is a major measure
that helps reduce the spread of the diseases in new couples. So the government
should make it a law and anyone who has HIV should be rejected and killed, so
that he/she does not spread it to others»
(A 45-year-old mother: FGD of Traditionalists
mothers/Ampoma)
|
Less than half (37%) of respondents knew of someone or couple
who underwent a HIV PCT before marriage.
Large majority of both males (84.4%) and females (86.3%)
recognized that both partners are required to undergo PCT.
Also majority of respondents in both sexes (85.3%) knew the
first main advantage of HIV PCT (To know about their health and HIV status so
that they decide responsibly about marriage), less than half of them knew the
2nd advantage (To ensure stability and safety in marriage) [45%] and
the 3rd one (It strengthens marital relationship and enhances
marriage satisfaction) [29%], with few of them (14%) considering HIV PCT
advantage is to ensure fertility in couples.
|
«Oh yes! Premarital counseling and testing on
HIV is useful. It helps you to know your status regarding HIV. It advises us on
how to behave afterwards. It also strengthens marriage relationship and
faithfulness in couples. It is like an exam. When you don't want to become
last and you find out that you don't have HIV, you wouldn't like to fornicate
again». (A 25-year-old mother: FGD of traditionalist
mothers/Ampoma)
|
4.1. SCORE OBTAINED ON AWARENESS AND KNOWLEDGE
OF
RESPONDENTS ON HIV PCT
Using a scale of measurement described in point 3.6.2.3 ,
Findings in Table 5 suggest that as a whole, all different groups of
respondents in different categories (age group, residence, sub-districts, sex,
occupation, religious group, ethnic group, educational level..) had
Good knowledge on HIV PCT since none of the categories ranked
below the cut-off mean score of 11 below which we would consider there is poor
knowledge. Majority of different groups described in Table 5 fell in Average
Good Knowledge, except 3 groups which fell into Adequate Good knowledge (AKAN,
SSS and Post-middle college respondents). The mean score of knowledge for the
whole sample was 15.72 [SD2.8], falling in average level. Most mean scores in
different categories studied in table 5 varied between 14.4 and 17.5 (over the
total score 22 ) and did not show big significant differences between them,
meaning the adequacy of knowledge on HIV PCT seems similar in all these
different groups. . Only one category had a mean score corresponding to the
cut-off point (Respondents of post-secondary school level with a mean score of
11).
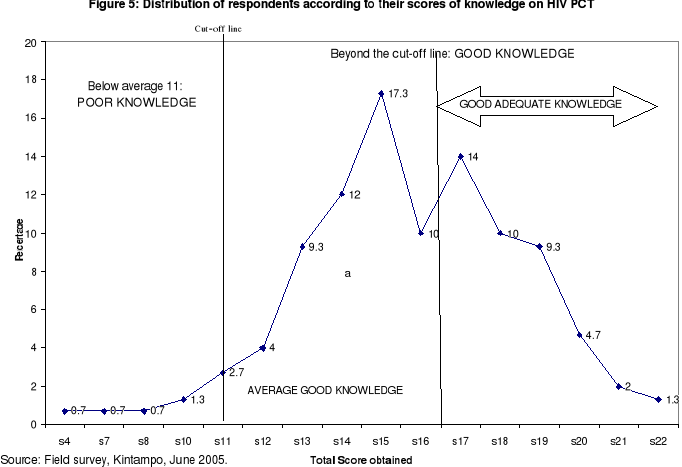
Also when one considers the individual scores as it is shown
in Figure 5 below, large proportion of respondents (97 % beyond the cut-off
line from average score 11 and over) proved «Good Knowledge»
(GK) on HIV PCT, with 41.3% scoring «Adequate Good
Knowledge» versus 55.7% scoring «Average Good
Knowledge». On the other hand a minority of respondents proved
«Poor Knowledge» (3 % below average score 11). The
trend shows a right skewed distribution with a peak at score 15 (17.3%), then
the number of respondents gradually decreases as the score increases, with few
people scoring the maximum (1.3%).
|
Table 5: Level of knowledge on HIV PCT among
respondents
|
|
Background characteristic
|
Total score computed in the whole(n)
|
Range score obtained
|
Mean score obtained (u) [SD]
|
Conclusion on level of knowledge*
|
|
Age : 15-19
|
942 (n=61)
|
7-22
|
15.4[SD=2.87]
|
Average GK
|
|
21-24
|
843 (n=53)
|
10-22
|
15.9[SD=2.54]
|
Average GK
|
|
25-30
|
574 (n=36)
|
4-21
|
15.9[SD=3.94]
|
Average GK
|
|
|
|
|
|
|
Residence: Urban
|
1673(n=107)
|
4-22
|
15.6[SD=2.9]
|
Average GK
|
|
Rural
|
686 (n=43)
|
11-22
|
15.9[SD=2.8]
|
Average GK
|
|
|
|
|
|
|
Sub districts: K'po
|
1259(n=81)
|
4-22
|
15.5[SD=2.7]
|
Average GK
|
|
JH
|
672(n=41)
|
7-22
|
16.4[SD=3.3]
|
Average GK
|
|
NL
|
428(n=28)
|
11-19
|
15.3[SD=2.3]
|
Average GK
|
|
|
|
|
|
|
Sex M
|
1208(n=77)
|
4-22
|
15.68[SD=2.6]
|
Average GK
|
|
F
|
1151(n=73)
|
7-22
|
15.76[SD=3.1]
|
Average GK
|
|
|
|
|
|
|
Educ. level: None
|
489(n=32)
|
11-20
|
15.2[SD=2.26]
|
Average GK
|
|
Primary
|
393(n=27)
|
8-20
|
14.5[SD=2.75]
|
Average GK
|
|
Middle/JSS
|
844(n=54)
|
7-22
|
15.6[SD=2.83]
|
Average GK
|
|
Tech/SSS/sec sch
|
544(n=31)
|
14-22
|
17.5[SD=2.15]
|
Adequate GK
|
|
Post.mid college
|
69 (n=4)
|
15-20
|
17.2[SD=2.06]
|
Adequate GK
|
|
Post secondary S.
|
22 (n=2)
|
4-18
|
11[SD=9.89]
|
Average GK
|
|
Occupation: Farmer
|
365(n=24)
|
11-22
|
15.2[SD=2.8]
|
Average GK
|
|
Gov.Workers
|
58(n=4)
|
4-22
|
14.5[SD=7.59]
|
Average GK
|
|
Trader
|
334(n=20)
|
12-21
|
16.7[SD=2.6]
|
Adequate GK
|
|
Student
|
854(n=54)
|
10-21
|
15.8[SD=2.3]
|
Average GK
|
|
Others
|
748(n=48)
|
7-20
|
15.5[SD=2.94]
|
Average GK
|
|
Religion Christian
|
1558(n=98)
|
4-22
|
15.9[SD=2.9]
|
Average GK
|
|
Moslem
|
649 (n=42)
|
8-21
|
15.4[SD=2.57]
|
Average GK
|
|
None
|
151(n=10)
|
12-22
|
15.1[SD=2.96]
|
Average GK
|
|
Tribe: Akan
|
867(n=50)
|
4-22
|
17.3[SD=3.3]
|
Adequate GK
|
|
Mo
|
640(n=41)
|
11-19
|
15.6[SD=1.8]
|
Average GK
|
|
Others
|
852(n=59)
|
8-20
|
14.4[SD=2.8]
|
Average GK
|
|
Total sample
|
2359 n=150)
|
4-22
|
15.72 [SD2.8]
|
Average GK
|
|
*Note: Scale of measurement of level of knowledge on HIV PCT=
|
|
If u < 11: POOR knowledge (PK)
If u = 11: GOOD Knowledge (GK),
|
|
11-16.5: Average GK and >16.5:
Adequate GK.
|
|
Source: Field survey, Kintampo, June 2005.
|
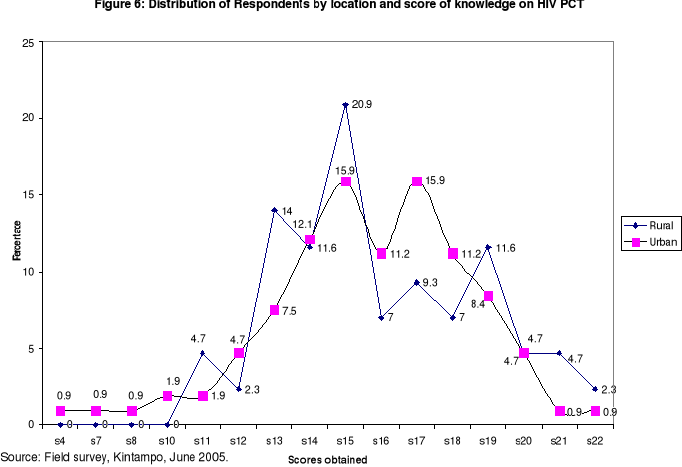
In figure 6, we see that respondents from rural parts knew
slightly more about HIV PCT than those coming from urban area, with the minimum
score of 11 and a mean score of 16.5 for rural respondents versus a minimum
score of 4 and a mean score of 13 among urban respondents. However the
difference in the trends of scores of knowledge between the two groups was not
statistically significant (p-value=0.25). The peak score was 15 among rural
respondents (20.9%) versus 2 peak scores of 15 (15.9%) and 17 (15.9%) among
urban respondents. Higher proportion of respondents who got maximum score of 22
were from rural parts (2.3%) as compared to those from urban ones (0.9%).
4.5. GENERAL PERCEPTION OF RESPONDENTS TOWARDS HIV
PCT
Findings in Table 6 below summarize the trend of how
respondents perceived HIV/AIDS and HIV PCT when the survey was carried out. The
following observations can be highlighted:
Large majority of Male (92.2%) as well as female (94.5%)
respondents perceived that although healthy they or their fiancé(e)s
could be unknown carrier of HIV AIDS. Females presented a slight higher risk
perception than males although there is no significant statistical difference
(p=0.81). This perception was expressed as well in FGDs carried out:
|
«Because of money, a woman forced her
daughter to marry a man who came from London. This man was apparently healthy.
But who knew he was having it? Just 2 years and six months later he started
showing the symptoms and later died. The poor lady is also dying».(A
27-year-old boy: FGD Christian young adults)
|
|
Table 6: Trend of general perception of respondents towards
HIV PCT
|
|
Indicators on perception towards HIV
PCT
|
Yes (%)
Male
(N=77)
|
Yes (%)
Female
(N=73)
|
Yes (%)
Total
(N=150)
|
p-value
X2*
OR
|
|
1.Perceive that one or one's partner [fiancé (e)]
though
apparently healthy can be an unknown carrier of
HIV/AIDS that could be detected during PCT
(Risk perception)
|
71
(92.2)
|
69
(94.5)
|
140
(93.3)
|
OR=0.7
p=0.81
|
|
2.Perceive that HIV-AIDS is a very dangerous/fatal disease
(Perceived severity of HIV/AIDS)
|
77
(100.0)
|
73
(100)
|
150
100.0
|
-
|
|
3.Perceive that there is a high risk of getting married
unknowingly to an HIV infected person and of becoming
HIV infected when two fiancés do not attend any
premarital medical examination on HIV test (Perceived
threat of contracting HIV in case one marries without
attending HIV PCT)
|
74
(96.1)
|
73
(100)
|
147
98.0
|
-
|
|
4.Believe that HIV Premarital Counseling and Testing
(PCT) is important (Perceived benefit of HIV PCT)
|
77
(100.0)
|
73
(100.0)
|
150
(100.0)
|
-
|
|
5.Believe they are self-confident and able to decide
themselves to undergo HIV PCT (Perceived self efficacy
towards HIV PCT)
|
76
(98.7)
|
71
(97.3)
|
147
(98.0)
|
-
|
|
6.Believe that their family will support them or encourage
them to perform HIV PCT before getting married
(perceived HIV PCT as a subjective -family norm a)
|
75
(97.4)
|
69
(94.5)
|
144
(96.0)
|
-
|
|
7. Believe that their family will support them or
encourage
them to perform HIV PCT before getting married
(perceived HIV PCT as a subjective-peer norm b)
|
71
(92.2)
|
60
(82.2)
|
131
(87.3)
|
OR=2.5
p=0.11
|
|
8. Perceive that HIV PCT should be institutionalized in the
district (Perceived HIV PCT as a social norm)
|
76
(98.7)
|
72
(98.6)
|
148
(98.7)
|
OR=1.0
p=0.5
|
|
8.1.Perceive that HIV PCT should be made
compulsory
|
48 (63)
|
42(58)
|
90(61)
|
OR=1.2
p=0.66
|
|
8.2.Perceive that HIV PCT should be made
optional
|
28(37)
|
30(42)
|
58(39)
|
|
9. Perceive there are some barriers to HIV PCT acceptance
and implementation in Kintampo (perceived barrier to
HIV PCT)
|
61
(79.2)
|
60
(82.2)
|
121
(80.7)
|
OR=0.8
p=0.79
|
|
10. Perceive there is the need of implementing HIV PCT
services in Kintampo district in the fight against
HIV/AIDS in new couples (Perceived need of HIV PCT
services)
|
76
(98.7)
|
73
(100.0)
|
149
(99.3)
|
-
|
|
11. Have the willingness to undergo HIV PCT with their
fiancé (e) before Marriage.
|
75
(97.4)
|
72
(98.6)
|
147
(98.0)
|
-
|
|
12. Perceive they are ready to know and accept their HIV
test result after HIV PCT
|
75
(97.4)
|
70
(95.9)
|
145
(96.7)
|
-
|
|
[Chi-Square, Note: X2(Y)=Yates corrected
chi-square, p<0.05, CI:95%]
|
|
Source: Field survey, Kintampo, 2005.
|
The totality of respondents (100%) in both sexes perceived the
severity of HIV/AIDS and subsequently also perceived perfectly the importance
of HIV PCT. Also most of them perceived the threat of contracting HIV/AIDS in
case they marry without performing the HIV test. This trend also emerged from
qualitative discussions:
|
«In this time of HIV/AIDS, there are no more
jokes in marriage matters. HIV/AIDS has totally limited the freedom and the
right of people to marry. Because of HIV/AIDS you have to carefully choose your
marriage partner. And the right way to do it is to perform HIV test before you
go ahead. Meeeeeee! (with strong gesture), I cannot marry a HIV partner. God
forbid!»
(A 22-year-old single girl: FGD Moslem
girls)
|
Large majority of respondents in both sexes (98%) believed
they were able personally to perform HIV PCT.
|
«It is the matter of my own life.
Irrespective of whatever views from people or family members , me I know I have
to perform HIV test before marriage, so that I guarantee a bright future in my
family»
(A 24-year-old girl: FGD Christian young
adult).
|
Large majority of respondents perceived that the family
members and peers could support and encourage them towards HIV PCT.
Large majority of respondents (98.7%) in the survey perceived
HIV PCT should be institutionalized in Kintampo District, with the majority
(61%) perceiving it should be compulsory versus the minority (39%) saying it
should be optional rather.
This is supported by findings from qualitative study where
almost majority of participants opted HIV PCT should be compulsory with a few
of them opting it should be optional.
Respondents of both sexes almost universally perceived the
need of implementing HIV PCT services in Kintampo District (99.3%) although
they also recognized there were some barriers to its implementation and
acceptance (80.7%).
|
«It has to be implemented. If so it will help
those who understand its importance. Barriers are for those who just don't make
an effort to understand its usefulness. So instead of leaving two people to
death, it's better to save one of them. Therefore this service is needed since
it will save so many lives».
( A 24-year-old girl: FGD Moslem
girls).
|
Finally Table 6 shows that almost all the respondents in both
sexes had the willingness to undergo HIV PCT before their marriage (98.0%) and
said they were ready to know and accept their HIV test results after PCT
(96.7%).
The general trend showed no significant difference of views in
males and females, meaning they similarly perceived HIV PCT.
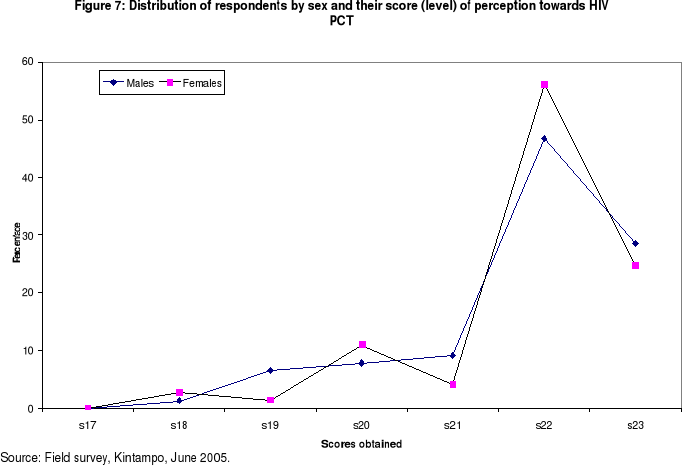
4.6. SCORES OBTAINED ON PERCEPTIONS OF RESPONDENTS
TOWARDS HIV PCT
Using a scale of measurement described in point 3.6.2.3 (see
Methodology), Table 7 and Figure 7 show that the entire totality (100%) of
respondents in both sexes had «adequate positive
perception» towards HIV PCT irrespective of their
different socio-demographic backgrounds , the minimum score obtained being 18,
with a mean score of 21.81 (SD=1.16 ). The curve is right skewed with no great
difference between males (mean score= 21.7[SD=1.2]) and females (mean score=
21.8[SD=1.13]). 20-28% of respondents scored the maximum of 23 marks.
|
Table 7: Level of perception towards HIV PCT among
respondents
|
|
Background characteristic
|
Total score computed in the whole(n)
|
Range score obtained
|
Mean score obtained (u) [SD]
|
Conclusion on level of perception*
|
|
Age : 15-19
|
1333 (n=61)
|
19-23
|
21.8[SD=1.04]
|
AP
|
|
21-24
|
1160 (n=53)
|
18-23
|
21.8[SD=1.12]
|
AP
|
|
25-30
|
779 (n=36)
|
18-23
|
21.6[SD=1.4]
|
AP
|
|
Residence: Urban
|
2334(n=107)
|
18-23
|
21.8[SD=1.3]
|
AP
|
|
Rural
|
938 (n=43)
|
18-23
|
21.8[SD=1.07]
|
AP
|
|
Sub Districts: K'po
|
1751(n=81)
|
18-23
|
21.6[SD=1.09]
|
AP
|
|
JH
|
913(n=41)
|
19-23
|
22.2[SD=0.9]
|
AP
|
|
NL
|
608(n=28)
|
18-23
|
21.7[SD=1.4]
|
AP
|
|
Sex: M
|
1678(n=77)
|
18-23
|
21.7[SD=1.2]
|
AP
|
|
F
|
1594(n=73)
|
18-23
|
21.8[SD=1.13]
|
AP
|
|
Educational level:
None
|
720(n=32)
|
18-23
|
21.8 [SD=1.18]
|
AP
|
|
Primary
|
591(n=27)
|
19-23
|
21.8[SD=1.12]
|
AP
|
|
Middle/JSS
|
1151(n=54)
|
18-23
|
21.7[SD=1.3]
|
AP
|
|
Tech/SSS/sec sch
|
679(n=31)
|
19-23
|
21.9[SD=0.87]
|
AP
|
|
Post.mid college
|
89 (n=4)
|
21-23
|
22.5[SD=0.9]
|
AP
|
|
Post secondary S.
|
42 (n=2)
|
19-23
|
21[SD=2.8]
|
AP
|
|
Occupation: Farmer
|
524(n=24)
|
19-23
|
21.8[SD=1.27]
|
AP
|
|
Gov.Workers
|
86(n=4)
|
19-23
|
21.5[SD=1.7]
|
AP
|
|
Trader
|
432(n=20)
|
18-23
|
21.6[SD=1.3]
|
AP
|
|
Student
|
1175(n=54)
|
19-23
|
21.7[SD=1.1]
|
AP
|
|
Others
|
1055(n=48)
|
18-23
|
21.9[SD=1.08]
|
AP
|
|
Religion: Christian
|
2158(n=98)
|
18-23
|
21.7[SD=1.16]
|
AP
|
|
Moslem
|
893 (n=42)
|
18-23
|
21.7[SD=1.19]
|
AP
|
|
Others
|
221(n=10)
|
20-23
|
22.1[SD=1.19]
|
AP
|
|
Tribe: Akan
|
1096(n=50)
|
18-23
|
21.9[SD=1.04]
|
AP
|
|
Mo
|
908(n=41)
|
18-23
|
21.6[SD=1.3]
|
AP
|
|
Others
|
1268(n=59)
|
18-23
|
21.8[SD=1.16]
|
AP
|
|
Total sample
|
3272 n=150)
|
18-23
|
21.8[SD=1.16]
|
AP
|
|
*Note: Scale of measurement of level of perception on HIV
PCT=
If u < 11.5: Negative or bad perception
If u = 11.5: Positive (high, good)perception:
11.5-17.5: Average Positive perception and
>17.5=Adequate Positive perception (AP)
|
|
Source: Field Survey, Kintampo, June 2005.
|
4.7. RELATIONSHIP BETWEEN SCORE OF KNOWLEDGE AND SCORE
OF
PERCEPTION AMONG
RESPONDENTS.
As it can be implied in Table 8 below, there was a weak
positive linear relationship between the two variables which was statistically
significant (p-value 0.007). The score of perception slightly
increases as the score of knowledge increases. But even respondents with poor
score of knowledge also had higher score of perception.
|
Table 8: Linear Regression: Regress score of perception
=score of knowledge, CL =95%
|
|
Linear Regression: Regress Pscore=Kscore p-value
=95%
|
|
Variable
|
Coefficient
|
Std Error
|
F-test
|
P-Value
|
|
Score of knowledge
|
0.088
|
0.032
|
7.4156
|
0.007
|
|
CONSTANT
|
20.422
|
0.519
|
1545.6573
|
0
|
|
Correlation Coefficient: r^2=0.05
|
|
Source
|
df
|
Sum of Squares
|
Mean Square
|
F-statistic
|
|
Regression
|
1
|
9.675
|
9.675
|
7.416
|
|
Residuals
|
148
|
193.098
|
1.305
|
|
|
Total
|
149
|
202.773
|
|
|
|
Source: Field survey, Kintampo, June 2005.
|
From Table 8, we derived the model of the form: Y=
á + ßX, where Y is the score of perception and X the
score of knowledge towards HIV PCT.
The regression straight line fits to the following model:
Y=20.422+0.088X
Using this modal we could predict the score of perception of
any unmarried young adults based on his/her score of knowledge in answering to
the defined questions in the questionnaire. Thus for instance a respondent with
a score of knowledge of 10 would have a score of perception of 21.302.
4.8. FACTORS INFLUENCING PERCEPTION OF THE NEED OF HIV
PCT
SERVICES
|
Table 9. Factors (predictors) influencing Perceived
need of HIV PCT service (p1) among unmarried young adults in
Kintampo District
|
|
Variables
|
Coefficient
|
SE
|
Z-test*
|
p-value
>Z
|
Odds ratio
(95%CI Odds ratio)
|
|
Intercept (constant á1 )
|
-35.38
|
21.29
|
-1.6
|
0.096
|
-
|
|
Socio-Demographic Background:
(X1) Age
|
0.2983
|
0.3082
|
0.967
|
0.333
|
1.3 (0.7, 2.5)
|
|
(X2)Sex (Female)
|
2.975
|
2.131
|
1.39
|
0.16
|
19.5 (0.3, 1278)
|
|
(X3)Place of residence (Urban)
|
-1.622
|
2.366
|
-0.68
|
0.492
|
0.19 (0.002, 20.4)
|
|
(X4) Religious group (Christian)
|
1.717
|
2.516
|
0.68
|
0.49
|
5.57 (0.04, 773)
|
|
(X5)Ethnic group (Akan & Mo)
|
1.0331
|
2.5015
|
0.413
|
0.679
|
2.8 (0.02, 378.4)
|
|
(X6) Level of education (Post Primary)
|
1.418
|
2.446
|
0.57
|
0.56
|
4.13 (0.03, 500)
|
|
(X7) Profession (Student/Pupil)
|
1.4105
|
2.995
|
0.470
|
0.637
|
4.097(0.01, 1452.1)
|
|
(X8) Premarital sex history : Have had
premarital sex (Yes)
|
-2.727
|
2.768
|
-0.98
|
0.324
|
0.06 (0.0003, 14.8)
|
|
(X9) SCORE (LEVEL) OF KNOWLEDGE
ON HIV/ PCT**
|
-0.017
|
0.375
|
-0.04
|
0.96
|
0.98 (0.47, 2.1)
|
|
(X10) SCORE (LEVEL) OF PERCEPTION
TOWARDS HIV/PCT**
|
1.4974
|
0.8998
|
1.664
|
0.096
|
4.47 (0.8, 26.1)
|
|
*Z-test, p-value<0.05 , ** See ANNEX 5 to view variables
used in scoring scales
|
|
Logit Model: Ln[p1/ (1-
p1)]=-35.38+0.2983 X1+ 2.975X2-1.622
X3 + 1.717X4 +1.0331X5
+ 1.418X6 +1.4105X7
-2.727X8 - 0.017X9
+1.4974X10
|
|
Source: Field survey, Kintampo, June 2005.
|
Although there is no significant association between dependant
variable and explanatory variables under study, Table 9 above demonstrates the
following:
1. Perception of the need of HIV PCT was inversely
(negatively) associated with Urban residence, with the fact of having had
premarital sex and with score (level) of knowledge.
2. Perception of the need of HIV PCT service was positively
associated with increased level of perception towards HIV PCT, age, being
female, Christian, being of Akan and Mo ethnic group, being of post-primary
educational level and being student.
4.9. FACTORS INFLUENCING WILLINGNESS TO UNDERGO HIV
PCT
Table 10 below shows that there was only one reliable positive
predictor of willingness to undergo HIV PCT. This predictor was the readiness
of a respondent to know and accept his/her HIV result. In fact willingness to
undergo HIV PCT was strongly associated with readiness of a respondent to know
and accept his/her HIV result (p<0.001), with Odds ration
far exceeding the constant (1 x constant E12= 162754.79).
|
Table 10. Factors (predictors) influencing willingness
to undergo HIV PCT service (p2) among unmarried young adults in
Kintampo District
|
|
Variables
|
Coefficient
|
SE
|
Z-test*
|
p-value
>Z
|
Odds ratio
(95%CI Odds ratio)
|
|
Intercept (constant á2 )
|
-39.715
|
15.934
|
-2.5
|
0.0127
|
*
|
|
Socio-Demographic Background:
(X'1) Age
|
-0.0296
|
0.1839
|
-0.2
|
0.8722
|
0.9 (0.7,1.4)
|
|
(X'2)Sex (Female)
|
1.2901
|
1.252
|
1.03
|
0.3028
|
3.6 (0.3,42.3)
|
|
(X'3)Place of residence (Urban)
|
1.1279
|
1.3789
|
0.8
|
0.4134
|
3.1(0.2, 46.1)
|
|
(X'4) Religious group (Christian)
|
1.2919
|
1.5037
|
0.86
|
0.3903
|
3.6 (0.2, 69.3)
|
|
(X'5) Ethnic group (Akan & Mo)
|
0.9243
|
1.4945
|
0.62
|
0.5363
|
2.5 (0.1, 47.1)
|
|
(X'6) Level of education
(Post Primary)
|
-1.2049
|
1.434
|
-0.84
|
0.4008
|
0.3 (0.01, 5.0)
|
|
(X'7) Profession (Student)
|
-0.3604
|
1.7713
|
-0.2
|
0.8387
|
0.7 (0.02,22.4)
|
|
(X'8) Premarital sex history : Have had
premarital sex (Yes)
|
-1.5237
|
1.6286
|
-0.9
|
0.3495
|
0.2 (0.01,5.3)
|
|
(X'9) SCORE (LEVEL) OF KNOWLEDGE ON HIV/
PCT**
|
0.1913
|
0.2191
|
0.9
|
0.3826
|
1.2 (0.8, 1.9)
|
|
(X'10) SCORE (LEVEL) OF PERCEPTION TOWARDS
HIV/PCT**
|
0.7263
|
0.5674
|
1.3
|
0.2006
|
2.1(0.7, 6.3)
|
|
(X'11) Perceived need of HIV PCT
service (Yes)
|
-3.1371
|
7.3989
|
-0.4
|
0.6716
|
0.04 (0.0, 86196)
|
|
(X'12) Perceived need of confidentiality and
privacy in HIV/PCT service.
|
0.9644
|
7.5131
|
0.13
|
0.8979
|
2.6(0,6516187)
|
|
(X'13) Readiness to know and accept
HIV PCT Results (Yes)
|
28.3658
|
3.605
|
7.9
|
<0.001
|
>162755
(14423,>162755)
|
|
(X'14) Suggestion that HIV PCT service should be
provided free of charge (yes)
|
-0.8604
|
4.2528
|
-0.2
|
0.8397
|
0.4(0.0001,1763.26)
|
|
*Z-test, p-value<0.05, ** See ANNEX 5 to view variables
used in scoring scales.
|
|
Logit Model: Ln[p2/(1-
p2)]= -39.715-0.0296X'1+
1.2901X'2-1.1279X'3 + 1.2919X'4
+0.9243X'5 -1.2049X'6
-0.3604X'7 -1.5237X'8 +
0.1913X'9 +0.7263X'10-3.1371X'11
+0.9644X'12 +28.3658X'13
-0.8604X14
|
|
Source: Field survey, Kintampo, June 2005.
|
Other no significant associations are as follows:
1. Willingness to undergo HIV PCT was negatively associated
with age, post-primary educational level, being student, having ever had
premarital sex, perceiving the need of HIV PCT services and suggestion that HIV
PCT should be provided free of charge.
2. Willingness to undergo HIV PCT was slightly positively
associated with Akan & Mo Ethnic groups, urban residence, Christian
religion, female sex, score (level) of knowledge, and score (level) of
perception towards HIV PCT and suggestion of confidentiality in PCT
services.
4.10. DEDUCTION OF PROBABILITY FOR RESPONDENTS TO
PERCEIVE THE NEED OF HIV PCT SERVICE AND TO INTEND UNDERGOING HIV
PCT
|
Table 11: Distribution of respondents according to
their probability of perceiving the need of HIV PCT service and of willingness
to undergo HIV PCT
|
|
Probability for willingness to undergo HIV PCT
|
|
|
0-0.5
|
>0.75
|
TOTAL
|
|
Probability for perceiving the need of HIV PCT service
|
0-0.5
|
1(0.67%)
|
5(3.33%)
|
6(4.00%)
|
|
0.6-0.75
|
2(1.33%)
|
10 (6.67%)
|
12 (8.00%)
|
|
> 0.75
|
3 (2.00%)
|
129 (86.00%)
|
132 (88.00%)
|
|
TOTAL
|
6(4.00%)
|
144(96.00%)
|
150 (100.00%)
|
|
Source: Field survey, Kintampo, June 2005.
|
Using the two logit models described in Tables 9 and 10, we
deduced the probability for each respondent to perceive the need of HIV PCT
service and the probability of willingness to undergo HIV PCT. Table 11 above
shows that 86% of respondents had a higher probability
(>0.75%) of perceiving the need of HIV PCT service (Mean probability:
0.923786) and of willingness to undergo HIV PCT (mean probability:
0.946193992).
4.11. PREFERENCE TO UNDERGO HIV VCT FOR MARITAL REASON
OR NOT
|
Table 12. Distribution of respondents by sex and HIV
testing choices
|
|
PREFERENCE
|
|
Sex
|
HIV PCT
(%)
|
VCT outside
Marriage context (%)
|
TOTAL
|
|
Female Female Female
|
58 (80)
|
15 (20)
|
73 (100.0)
|
|
Male
|
57 (74)
|
20 (26.0)
|
77 (100.0)
|
|
TOTAL
|
61 (77)
|
35 (23)
|
150 (100.0)
|
|
X2(Yates)=0.35, p-value 0.55, CL 95%, OR=1.36
|
|
Source: Field survey, Kintampo, June 2005.
|
Table 12 illustrates that majority of respondents
(77%) preferred undergoing HIV PCT while minority of them
(23%) preferred voluntary HIV testing outside marriage context. Table 12 does
not show any significant difference of preference choices given the sex of
respondents (p-value 0.55), the Odd ratio of preference of HIV PCT in females
being 1.36 times the odd in males.
4.12. BARRIERS TO HIV PCT ACCEPTANCE AND
IMPLEMENTATION
IN KINTAMPO
DISTRICT
Respondents were asked about what they think were the barriers
to HIV PCT acceptance and implementation in Kintampo District. A long list of
barriers was generated as shown in Table 13 below.
|
Table 13: Respondents' perception of barriers to HIV PCT
acceptance and implementation
|
|
No
|
Perceived Barriers to HIV PCT
|
Yes
(%)
|
No
(%)
|
NK
(%)
|
|
1
|
Inexistence of regulatory procedures and Law/Policy on PCT in
Ghana
|
90
(60.00)
|
59
(39.30)
|
1 (0.7)
|
|
2
|
Mandatory imposition of PCT that infringes the Human Right of
individuals
|
86
(57.3)
|
63
(42.00)
|
1
(0.7)
|
|
3
|
High cost (price) of premarital examinations
|
110
(73.3)
|
40
(26.7)
|
-
|
|
4
|
The location of the centre/hospital at long distances
|
94 (62.7)
|
56
(37.3)
|
-
|
|
5
|
The attitude of the service provider
|
116 (77.3)
|
34 (22.7)
|
-
|
|
6
|
Premarital sex and fear to know one's HIV status
|
110 (73.3)
|
40
(26.7)
|
-
|
|
No
|
Perceived Barriers to HIV PCT
(Continued)
|
Yes
(%)
|
No
(%)
|
NK
(%)
|
|
7
|
Fear of stigma and discrimination in marriage (denial of
marriage for HIV+)
|
116 (77.3)
|
33 (22.0)
|
1 (0.7)
|
|
8
|
Ignorance of the importance of PCT (illiteracy...)
|
111 (74.0)
|
39
(26.0)
|
-
|
|
9
|
Reluctance of fiancés
|
98 (65.3)
|
50 (33.3)
|
2 (1.3)
|
|
10
|
Preference of young people to get married without PCT
|
88 (58.7)
|
61 (40.7)
|
1 (0.7)
|
|
11
|
Opposition of some churches
|
71 (47.7)
|
78 (52.3)
|
-
|
|
12
|
Opposition of some parents
|
72 (48.0)
|
77 (51.3)
|
1 (0.7)
|
|
13
|
Polygyny (Polygynous/polygamous marriages)
& Islamic religion
|
78 (52%)
|
72 (48.0)
|
-
|
|
14
|
Marriage by convenience (outside churches & civil
registrar officer our court or without customary ritual)
|
94 (62.7)
|
55 (36.7)
|
1
(0.7)
|
|
15
|
Forced marriage (e.g. traditional early marriage)
|
93 (62.4)
|
56 (37.6)
|
-
|
|
16
|
Unregistered marriage
|
81 (54.0)
|
60 (46.0)
|
-
|
|
17
|
Inadequate VCT/PCT facilities
|
109 (72.7)
|
41 (27.3)
|
-
|
|
18
|
Lack or inadequate trained personnel & counselors
|
107 (71.3)
|
43 (28.7)
|
-
|
|
19
|
Fiancés are in a hurry to get married very quickly for
any reason
|
91 (60.7)
|
58 (38.7)
|
1 (0.7)
|
|
20
|
Lack of confidentiality and privacy among health care
providers in PCT services.
|
109 (72.7)
|
41 (27.3)
|
-
|
|
21
|
Medical premarital certificate provided to fiancé(e) by
doctors without performing any medical check-ups (fraud)
|
97 (64.7)
|
53 (35.3)
|
-
|
|
22
|
Re-marriage ( for divorced or widowed)
|
84 (56.0)
|
66(44.0)
|
-
|
|
23
|
Inability for girls to negotiate for HIV PCT when boys don't
like it
|
100 (67.1)
|
49 (32.9)
|
-
|
|
24
|
Little solution for those who test HIV (+) ( no effective
drugs to treat AIDS)
|
106 (70.7)
|
44 (29.3)
|
-
|
|
25
|
Blind love among young people
|
85 (56.7)
|
64 (42.7)
|
1 (0.7)
|
|
26
|
Others (not providing gifts to couples, ...)
|
26 (17.4)
|
111 (74.5)
|
12 (8.1)
|
|
NK=Not known (Don't know)
Source: Field survey, Kintampo, June 2005.
|
For easier interpretation perceived barriers described in
Table 13 could be grouped under 4 categories:
1. Major absolute barriers: the proportion of respondents who
said yes is =70%.
These are barriers number 3, 5, 6, 7, 8, 17, 18, 20 and 24.
2. Moderate barriers: the proportion of respondents who said
yes is between 50-69%.
These are barriers number 1, 2, 4, 9, 10, 13, 14, 15, 16, 19,
21, 22, 23 and 25.
3. Minor barriers: the proportion of respondents who said yes
is between 30-49 %. These are barriers number 11and 12
4. Negligible barriers: the proportion of respondents who said
yes is < 30%.
Barriers grouped under «others» in index number 26
fit to this category.
Some of these barriers were also recognized in qualitative
study as it can be related in the following quotes.
|
«Since there is no official law on premarital
examinations here in Ghana which would enable people to test before marriage,
many people marry without testing and thus become victims of many diseases such
as HIV/AIDS which, yet, could have been prevented.»
(IDI: District AIDS Initiative
coordinator/DA/GES/Kintampo, Picture No 9).
|
|
|
«We know that premarital counseling and testing is
part of reproductive health. But we haven't started a special service on it
yet. But things are in the pipe so that a VCT and premarital counseling service
would be implemented in the District»
(IDI :Public Health Nurse and Responsible of Family Health
Clinic/Kintampo)
|
|
«Many young adults have had premarital sex and
because of that they fear to go for the HIV PCT»
(A 4- year-old mother: FGD of Traditionalist
mothers/AMPOMA)
|
|
«Some girls have stayed long without getting men to
marry and when a man promises to marry such girl, she may want the marriage to
happen in no time because she thinks the man may see an other woman and change
the decision, or the test result may compromise the marriage. So in her plan
marriage without any ado with no ceremonial medical examinations is just the
best to satisfy her over due dreams. I am among this group. Just understand
this. Isn't it?»(A 23-year-old girl: FGD Moslem Girls)
|
|
«Broadcasting of the HIV test results in hospitals
and in the public is a major obstacle to HIV PCT. If you want it to work, bring
us counselors who are not known locally or may be people can go and test far in
other new places from their home towns. I don't talk about stigma and
discrimination which are also there.»
(A 39-year-old man: FGD Moslem fathers).
|
Since during FGD of Moslem girls participants also recognized
their religion as a barrier to HIV PCT implementation we found better to
stratify frequencies of this barrier over religion background.
Table 14 below shows that 43.9 % of Moslem
respondents also mentioned Islam as a barrier to HIV PCT. Though statistically
insignificant, there is some level of association between religion and
perception of Islam as a barrier to HIV PCT (p-value = 0.08), meaning Moslem
and non Moslem respondents perceive in the same way that Islam is a barrier to
HIV PCT.
|
Table 14: Distribution of respondents by religion and
perception of
Islam as a barrier to HIV PCT
implementation
|
|
Perceive Islam as a barrier to HIV PCT
|
|
|
Religion
|
Yes (%)
|
No (%)
|
TOTAL (%)
|
|
Catholic
|
15 (41.7)
|
21 (58.3)
|
36 (100.0)
|
|
Protestant
|
23 (63.9)
|
13 (36.1)
|
36 (100.0)
|
|
Pentecostal
|
19 (70.4)
|
8 (29.6)
|
27 (100.0)
|
|
Muslim
|
18 (43.9)
|
23 (56.1)
|
41 (100.0)
|
|
No Religion
|
5 (50.0)
|
5 (50.0)
|
10 (100.0)
|
|
TOTAL
|
80 (53.3)
|
70 (46.7)
|
150 (100.0)
|
|
X2: 8.2, p-value:0.08, CL 95%
|
|
Source: Field survey, Kintampo, June 2005.
|
4.13. KEY ISSUES FROM RESPONDENTS TOWARDS HIV PCT
HEALTH
PRACTICE IN KINTAMPO
DISTRICT
|
|

