Evaluation of the hypoglycemic, hypolipidemic and anti alpha amylase effects of extracts of the twigs and fruits of ficus ovata vahl (moraceae)( Télécharger le fichier original )par FOUONDO MAMETOU University of Yaoundé I - Master 2011 |

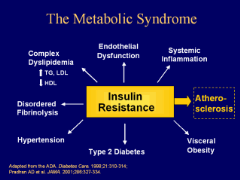
I.1.6.3. Other specific typesOther specific types are currently less common causes of diabetes mellitus, but are conditions in which the underlying defect or disease process can be identified in a relative specific manner (WHO, 1999). They include: - Genetic defects in ß-cells, such as maturity-onset diabetes of the young; - Genetic defects in insulin action, - Diseases of the exocrine pancreas, such as cancer of the pancreas, cystic fibrosis and fibrocalculous pancreatopathy (a form of diabetes that was formerly classified as one type of malnutrition-related diabetes mellitus) and many others. I.1.7. Complications of diabetes mellitusUncontrolled hyperglycemia in both type 1 and type 2 diabetes lead to the development of both acute and long term complications (Weiss and Sumpio, 2006).1(*) Acute complications of diabetes mellitus include ketoacidocis (type 1) or nonketotic hyperosmolar coma (type 2). Long term complications include cardiovascular diseases, hypertension, chronic renal failure, retinal damage, nerve damage, erectile dysfunction and macrovascular damage which may cause poor healing of wounds particularly of the feet and can lead to gangrene which may require amputation (WHO, 1999). Chronically elevated blood glucose levels lead to increase production of mitochondrial reactive oxygen species (ROS), which activate a number of metabolic pathways whose end products contribute to the development of long term complication of diabetes (Weiss et al., 2006). I.1.8. Diabetes mellitus in special groups and circumstancesI.1.8.1. Metabolic syndrome and type 2 diabetes mellitusOften a person with abnormal glucose tolerance (IGT or diabetes) will be found to have at least one or more of the other cardiovascular disease risk factors such as hypertension, central (upper body) obesity, and dyslipidemia. This clustering has been labelled diversely as the metabolic syndrome, syndrome X, or the insulin resistance syndrome (WHO, 2006). Alone, each component of the cluster conveys increased cardiovascular disease risk, but as a combination they become much more powerful. This means that the management of persons with hyperglycemia and other features of the metabolic syndrome should focus not only on blood glucose control but also include strategies to reduce the impact of other cardiovascular disease risk factors (WHO, 2006). The metabolic syndrome with normal glucose tolerance identifies the subject as a member of a group at very high risk of future diabetes. Thus, vigorous early management of the syndrome may have a significant impact on the prevention of both diabetes and cardiovascular disease, especially as it is well documented that the features of the metabolic syndrome can be present for up to 10 years before glycemia disorder is detected (Miller et al., 2010).
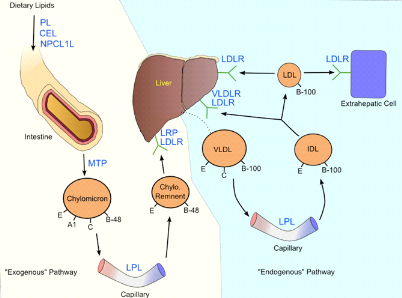
Figure 4 : Metabolic syndrome (Miller et al., 2010) I.1.8.2. Hyperlipidemia and type 2 diabetes mellitusHyperlipidemia refers to elevated levels of lipids and cholesterol in the blood, and is also identified as dyslipidemia, to describe the manifestations of different disorders of lipoprotein metabolism. Lipids in blood are either free or bound to other molecules. They are either provided by diet or are endogenously synthesized. Lipids, such as cholesterol and triglycerides, are insoluble in plasma. Circulating lipid is carried in lipoproteins that transport lipid to various tissues for energy use, lipid deposition, steroid hormone production and bile acid formation. The lipoprotein consists of esteri?ed and unesteri?ed cholesterol, triglycerides, phospholipids, and proteins. Abnormalities in lipoprotein metabolism are a major predisposing factor to atherosclerosis, increasing risk for CHD (Cromwell et al., 2006). Five major lipoproteins exist, each with a di?erent function: chylomicrons carry triglycerides from the intestine to the liver, skeletal muscles and to adipose tissues; very low density lipoproteins (VLDLs) carry (newly synthesized) triglycerides from the liver to adipose tissue; intermediate density lipoproteins (IDLs) are intermediate between VLDL and low density lipoprotein (LDL). LDL is the main carrier of circulating cholesterol within the body. It is used by extra hepatic cells for cell membrane and steroid hormone synthesis. Once the LDL is taken up by LDL receptors, free cholesterol is released and accumulates within the cells. High density lipoprotein (HDLs) collects cholesterol from body tissues and brings it back to the liver. The protein components of the lipoprotein are known as apolipoproteins or apoproteins. The different apolipoproteins serve as cofactors for enzymes, and ligands for receptors. Defects in apolipoprotein metabolism lead to abnormalities in lipid handling (Lucy et al, 2005). Three main pathways are responsible for the generation and transport of lipids within the body: exogenous, endogenous, and reverse cholesterol transport (Nicole et al., 2008). Although elevated low density lipoprotein cholesterol (LDLc) is thought to be the best indicator of atherosclerosis risk, dyslipidemia can also describe elevated total cholesterol (TC) or triglycerides (TG), or low levels of high density lipoprotein cholesterol (HDLc) (Cromwell et al., 2006). The most common lipid pattern in type 2 diabetes consists of hypertriglyceridemia, low high-density lipoprotein cholesterol (HDLc) and normal plasma concentrations of low-density lipoprotein cholesterol (LDLc). However, in the presence of even mild hyper-TG, LDLc particles are typically small and dense and may be more susceptible to oxidation (Grundy, 2006). Chronic hyperglycaemia promotes the glycation of LDLc and both these processes are believed to increase the atherogenicity of LDLc. Under normal circumstances, insulin activates the enzyme lipoprotein lipase and hydrolyses triglycerides. However, in insulin deficient subjects, it fails to activate the enzyme and causes hypertriglyceridemia. In insulin deficient diabetics, the plasma free fatty acid concentration is elevated as a result of increased free fatty acid outflow from fat depots, where the balance of the free fatty acid esterification-triglyceride lipolysis circle is displaced in favour of lipolysis (Jie et al., 2007). Excess plasma NEFA can inhibit insulin-stimulated glucose utilization in muscle and promote hepatic production of glucose. Whereas, reduction of plasma NEFA concentration improves glucose utilization, enhances the suppression of hepatic glucose production by insulin (Jie et al., 2007).
Figure 5 : Lipoprotein metabolism (Cromwell et al., 2006) * 1r disease in patients with diabetes mellitus". Eur J Vasc Endovasc Surg |
|