|



FACULTY OF MEDICINE
REVIEW OF GROIN HERNIAS AT KIBOGORA
HOSPITAL:
A retrospective descriptive study to describe the
prevalence, pattern and the immediate outcome of groin hernia surgery in
KIBOGORA Hospital, Department of surgery.
Dissertation presented in partial fulfillment of the
requirements for the
award of a degree of MB.ChB. of the National
University of Rwanda
Presented by:
Emile NDAHIRO
SUPERVISOR: Prof. Ignatius
KAKANDE
CO SUPERVISOR: Prof. Patrick
KYAMANYWA
HUYE, December 2008
DEDICATION
To the Almighty GOD,
For your Mercy, Grace and Love,
To my parents and grand parents,
Who very much wished to see me one day as a Doctor,
For your immeasurable love, tolerance, guidance and care, I
respect.
To all who are dear to me,
I dedicate this memoir.
ACKNOWLEDGEMENT
The success of a dissertation is a big endeavour that one
never claims to own alone and when it comes to expressing gratitude, it is
always hard to find who to thank and who to leave. This is because various
people played different roles under different circumstances in their particular
capacities through out the period of writing my dissertation. However let me
attempt to this great task:
I owe special thanks to my Mum SSONKO Prossy and Dad BIGIRANDE
Emile who managed to forego all and made their son an opportunity cost, without
forgetting my uncle MUGGAGA, brothers KAAYA, LUYIMA ,KAKANDE, ISHIMWE, SHYAKA
and my sisters NAMATOVU, NAKACHWA, UWASEKURU, and UMUBYEYI who were always
there for me during my academic struggle. May God bless them abundantly.
I extend my sincere gratitude to my supervisors Prof. Patrick
KYAMANYWA and Prof Ignatius KAKANDE, I am grateful for their advice,
instructions and time sacrificed towards the success of this work.
My heartfelt thanks go to Dr. George NTAKIYIRUTA for his
support towards perfecting my surgical skills during my spell in Kibogora
hospital, may GOD bless him endlessly.
I am greatly indebted to my friends more especially Fred,
Joseph, Ivan, James for their tireless help towards making this' dream `come
true.
There would be nothing unreasonable than not mentioning the
personal attention got from my beloved friends Rachael BUSINGYE and Bob KAGORO
for both moral and academic support.
Lastly I wish to thank the entire staff of the National
University of Rwanda; mostly the Faculty of Medicine may the almighty God award
you abundantly.
TABLE OF CONTENTS
DEDICATION
i
ACKNOWLEDGEMENT
ii
TABLE OF CONTENTS
iii
LIST OF FIGURES
v
LIST OF TABLES
v
ACRONYMS, INITIALS AND ABBREVIATIONS
vi
Old Hippocratic Oath 425 BC
vii
ABSTRACT
viii
CHAPTER 1: INTRODUCTION
1
CHAPTER 2: PROBLEM STATEMENT
3
2.1 Research question and objectives
4
2.1.1. Research question
4
2.1.2. Objectives
4
2.1.2.1. General objective
4
2.1.2.2. Specific objectives
4
CHAPTER 3: MATERIALS AND METHODS
5
3.1. Materials
5
3.1.1 Study design
5
3.1.2. Study Population and Site
5
3.1.3. Inclusion and exclusion criteria
5
3.1.4. Data collection
5
3.1.5. Data analysis methods
5
3.1.6. Ethical considerations
6
3.1.7. Study limitations
6
CHAPTER 4: RESULTS AND DISCUSSIONS
7
4.1. Results
7
4.1.1. Prevalence of Groin Hernia
7
4.1.2. Socio-demographic aspects
7
4.1.3. Clinical assessment
9
4.1.4. Analytical results
13
4.2. Discussion
15
A. Prevalence of Groin hernia in Kibogora Hospital
(Department of surgery)
15
B. Characteristics of patients according to age
15
C. Characteristics according to clinical
presentation and type/site of hernia
15
D. Characteristics of patients according to type of
operation
16
E. Anaesthesia
16
F. Post-operative complications/ evolution
17
CHAPTER 5. CONCLUSION AND RECOMMENDATIONS
18
5.1. CONCLUSION
18
5.2. RECOMMENDATIONS
18
REFERENCES
20
APPENDIX
22
LIST OF FIGURES
Figure 1: Prevalence of Groin hernia at KH
7
Figure 2: Distribution of patients basing on
Age
7
Figure 3: Distribution of patients basing on
Sex
8
Figure 4: Distribution of patients basing on the
mode of consultation
8
Figure 5: Distribution of patients basing on the
mode of their PMH
9
Figure 6: Distribution of patients basing on the
type of hernia
9
Figure 7: Distribution of patients basing on
pre-operative diagnosis
10
Figure 8: Distribution of patients basing on type
of operation
10
Figure 9: Distribution of patients basing on
anaesthesia
11
Figure 10: Distribution of patients basing on
post-operative stay
11
Figure 11: Distribution of patients basing on
post-operative complications
12
Figure 12: Distribution of patients basing on
condition on discharge
12
LIST OF TABLES
Table 1: Distribution of patients basing on
comparing sex and type of groin hernia
13
Table 2: Distribution of patients on comparing age
range and type of Groin hernia
13
Table 3: Distribution of patients basing on
comparing mode of consultation and Pre-operative diagnosis
14
Table 4: Distribution of patients basing on
comparison between previous medical status and post operative stay
14
ACRONYMS, INITIALS AND ABBREVIATIONS
COPD : Chronic Obstructive Pulmonary
Disease
DG : Diagnosis
FH : Femoral Hernia
GIT : Gastro Intestinal Tract
GUT : Genital Urinary Tract
IH : Inguinal Hernia
KH : Kibogora Hospital
LIH : Left Inguinal Hernia
NS : Non Significant
NUR : National University of Rwanda
RIH : Right Inguinal Hernia
S : Significant
SPSS : Statistical Package for Social
Sciences
Old
Hippocratic Oath 425 BC
I swear by Apollo the physician, and Aesculapius and Health
and all-heal, and all the gods and goddesses, that, according to my ability and
judgment, I will keep this oath and stipulation-to reckon him who taught me
this Art equally dear to me as my parents, to share my substance with him, and
relieve his necessities if required; to look upon his offspring in the same
footing as my own brothers, and to teach them this Art, if they shall wish to
learn it, without fee or stipulation, and that by percept, lectures and every
other mode of instruction, I will impart a knowledge of the Art to my own sons
and those of my teachers, and to disciple bound by a stipulation and oath
according to the law of medicine, but to none other.
I will follow that system of regimen, which, according to my
ability and judgment, I consider for the benefit of my patients, and abstain
from whatever is deleterious and mischievous.
I will give no deadly medicine to anyone if asked, nor suggest
such counsel; and in like manner I will not give to a woman pessary to produce
abortion. With purity and with holiness I will pass my life and practice my
Art.
I will not cut persons labouring under the stone, but will
leave this work to be done by men who are practitioners of this work.
Into whatever houses I enter, I will go into them for the
benefit of the sick and will abstain from every voluntary act of mischief and
corruption; and further from the seduction of female, or males, of freemen or
slaves.
Whatever in connection with my professional practice, I see or
hear, in the life of men, which ought not to be spoken of abroad, I will not
divulge, as reckoning that all such should be kept secret.
While I continue to keep this oath unviolated, may it be
granted to me to enjoy life and practice this Art, respected by all men, in all
times. Should I violate this oath may the reverse be my lot.
ABSTRACT
Background: Hernia is defined as
the protrusion of an organ or part of an organ or any other structure
through the wall of the cavity that normally contains it.
Goal: To determine the prevalence, pattern
and the immediate outcome of groin hernia surgery in Kibogora hospital.
Methodology: This was a retrospective
descriptive study for all patients treated for groin hernias in the period of
18 months from 01/01/2007 to 30/06 2008 at Kibogora hospital in the western
province. Data was collected using a structured data collection form from
patients' clinical files, computerized and analyzed using Epidata and SPSS
computer soft wares. The text was written using Microsoft word. Graphs, tables
and pie charts were drawn with the help of Microsoft excel. Results were
cross-tabulated to examine relationships and association between the variables.
Statistical analysis was performed using Q 2 for test of
association. P value of less than 0.05 was considered significant in all the
statistical tests performed.
Results: The Prevalence of GH in the surgical
department of Kibogora Hospital during the period of study was 121 (16%) among
the total of 765 cases. The Male: Female ratio occurrence was 6:1. In a total
of 121 cases, 105 (87%) were males and only 16 (13%) were females. Modified
Bassini was the most commonly applied technique in Groin Hernia repair (68%),
with spinal anesthesia being predominant (77%). Post-operative complications occurred in 25% of all
the cases and hematoma wound was the predominant (14%), scrotal edema followed
(7%) and wound sepsis came last with only a 4%. The majority of patients (78%)
were discharged in good condition
Conclusion: GH is a public health hazard at
large as revealed by the above results at Kibogora Hospital. Although the
majority of patients operated on for groin hernia are discharged in good
condition some post-operative complications (25%) were revealed, wound hematoma
and scrotal edema at 14% and 7% respectively were the common . Modified Bassini
technique and spinal anesthesia are commonly employed, though in our settings
local anesthesia is highly recommended.
Key words: groin hernia,
post-operative complications, evolution.
CHAPTER 1: INTRODUCTION
Hernia is the protrusion of an organ or part of an organ or
any other structure through the wall of the cavity that normally contains
it. 1,2Hernias (incorrectly known as rupture) are qualified by the
name of the part that protrudes or the area through which protrusion occurs.
Thus, an inguinal hernia, perhaps the most common form, is one that passes
through the abdominal wall in the groin area [1, 2].
There are two main types of groin hernias, inguinal and
femoral hernias.
Groin hernia may be either congenital or acquired. Congenital
hernias are preformed hernial openings caused by incomplete closure of the
abdominal wall (e.g., persistent processus vaginalis), while, in acquired
hernias, the cause is increasing dehiscence of fascial structure with
accompanying loss of abdominal wall strength. They develop typically in
locations where larger blood vessels or the spermatic cord lie, or where
previous incisions were made.
Different factors contribute to the etiology of groin hernias
such as increased intra-abdominal pressure (in pregnancy, heavy lifting,
chronic cough as in COPD, ascites, straining to pass stool, obesity)
[3] .
Symptoms of inguinal hernia may include a lump in the groin
near the thigh; pain in the groin; and, in severe cases, partial or complete
blockage of the intestine.
Blood may be unable to enter or leave the organs in a hernia,
so that they strangulate. This is more likely to happen in a hernia with a
narrow neck. Most strangulated hernias are therefore either inguinal or
femoral, because these hernias have narrow necks and they both require
immediate surgery. The main treatment for inguinal hernia in adults is surgery
to repair the weakness in the posterior wall. This surgery is called
herniorrhaphy. Sometimes the weak area is reinforced with prosthetic mesh. This
operation is called hernioplasty. In children usually the hernia sac is ligated
after reducing the hernia contents. If the protruding intestine becomes twisted
or traps stool, part of the intestine might need to be removed if
strangulated.
Femoral hernia is a variety of groin hernia. It usually
presents as a defect in the fascia transversalis that is exploited by a
peritoneal sac similar to the patent processus vaginalis in an indirect
inguinal hernia exploiting the deep ring in the fascia transversalis of the
posterior wall of the inguinal canal. Femoral hernias are not as common as
inguinal hernias. Femoral hernias are more common in women, usually elderly and
frail. They typically present as a groin lump. They may or may not be
associated with pain. Often, they present with a varying degree of complication
ranging from irreducibility through intestinal obstruction to strangulation of
contained bowel. The incidence of strangulation in femoral hernias is high. A
femoral hernia has often been found to be the cause of unexplained small bowel
obstruction [4].
CHAPTER 2: PROBLEM STATEMENT
Hernia repair is one of the most common operations performed
worldwide. However, the hernia burden in Rwanda remains unknown as does the
outcome of hernia repair surgery in our hospitals.
According to the National Centre for Health Statistics, about
700,000 inguinal hernia repairs are performed each year in the United States.
Surgery for hernias represents a significant social expenditure, particularly
when lost days of work are factored in. Direct annual costs of hernia surgery
alone have been estimated at (2.5 billion dollars). The indirect costs of
hernia surgery are difficult to determine, but clearly add substantially to the
overall costs [4].
In 2000 a prospective descriptive study was conducted at
Mulago National Referral and Teaching Hospital in Kampala Uganda for 12 months
and 208 patients under went surgical repair for groin hernia. There were 195
(93.7%) inguinal hernias of which 159 (81.5%) were indirect inguinal hernias
and 34 (17.4%) were of the direct inguinal variety. Busoga hernias were
diagnosed in only 4 (2.05%) of inguinal hernias. There were only 13 (6.2%)
femoral hernias. The pantaloon hernias were diagnosed in two patients
(1.1%).
One hundred and fifty (76.9%) of the inguinal hernia
presented as emergencies and 45 (23.1%) as elective. Post-operative
complications occurred in 41.8% of the cases. There was one death. (0.48%)
[5].
Femoral hernias are not as common as inguinal hernias. Femoral
hernias account for about 1.2% to 10% of all groin hernias. In British practice
50% of femoral hernias are admitted as emergencies with
strangulation2. In Nigeria, in a 5-year study done at a teaching
hospital, only 5 patients presented with femoral hernias out of a total of 111
groin hernias seen. In a 14-year period Miller, while working in different
parts of Kenya, saw only 3 cases of femoral hernias. He further noted that by
1961, no operation for femoral hernia appeared on the operation lists at
Kenyatta National Hospital in Nairobi[4].
A review of intestinal obstruction at Mulago Hospital between
1958 to 1960 showed that femoral hernias accounted for 12% of the strangulated
hernias. Whereas in Kampala, for every one man with a femoral hernia there are
nine women [5] the male to female ratio is 1.2 to 1 in the West
African Hausa [7] .
Untreated or recurrent groin hernias are responsible for an
incalculable loss of productivity and revenue. Postoperative convalescence also
contributes to absence from the work force.
Currently the epidemiology of groin hernias in Rwanda is not
well understood. This study aimed to evaluate the prevalence and possible
complications following surgery and gather baseline data for further clinical
and basic research on groin hernias in Rwanda. The study was also used to pass
on recommendations to different levels of decision making in government like
the ministry of health, Non-Government organizations, medical and paramedical
staff on better management and possible preventive measures for complications
encountered after groin hernia repair.
2.1 RESEARCH QUESTION AND OBJECTIVES
2.1.1. Research question
What is the prevalence and possible complications following
groin hernia surgery at Kibogora Hospital?
2.1.2. Objectives
2.1.2.1. General
objective
To determine the prevalence, pattern and the immediate outcome
of groin hernia surgery in Kibogora hospital.
2.1.2.2. Specific
objectives
(a) To determine the demographic characteristics of patients
presenting with specific type of groin hernia.
(b) Identification of the mode of presentation of groin
hernias.
(c) Report on the choice/mode of surgical repair.
(d) Report on the common complications seen after surgical
repair of GH.
CHAPTER 3: MATERIALS AND
METHODS
3.1. MATERIALS
3.1.1 Study design
This was a retrospective descriptive study; the study involved
a review of medical records of all patients treated for groin hernias in the
period of 18 months from 01/01/2007 to 30/06/ 2008 at Kibogora hospital.
3.1.2. Study Population and
Site
The study was carried out in the surgery
department of Kibogora Hospital, in the western province.
3.1.3. Inclusion and exclusion criteria
All patients diagnosed and admitted with Groin hernia as
(inguinal or femoral) and underwent hernia repair during 01/01/2007 to 30/06
2008 at Kibogora hospital. We exclude all incomplete files not providing the
key information.
3.1.4. Data collection
A structured data collection form was used during the review
of clinical files of the patients admitted to the hospital during the time
interval from 01/01/2007 to 30/06/2008 and this included; the patients'
registration data, clinical assessment, type of operation, type of anesthesia,
post operative stay in hospital, possible post operative complications and the
actual condition on discharge.
3.1.5. Data analysis methods
The text was written using Microsoft word. Graphs, tables and
pie charts were drawn with the help of Microsoft excel. The collected data was
computerized and analyzed using Epidata and SPSS computer soft wares, Results
were cross-tabulated to examine relationships and association between the
variables. Statistical analysis was performed using Q 2 for test of
association. P value of less than 0.05 was considered significant in all the
statistical tests performed.
3.1.6. Ethical considerations
No patient's name was written on the structured questionnaire
during the study and the data collected from patients' clinical files was
destroyed immediately after data analysis.
3.1.7. Study limitations
Our study was limited by the remote location of the hospital
in question. This had financial implications in terms of transport and
maintenance costs.
CHAPTER 4: RESULTS AND
DISCUSSIONS
4.1. RESULTS
4.1.1. Prevalence of Groin
Hernia
Figure 1: Prevalence of Groin
hernia at KH
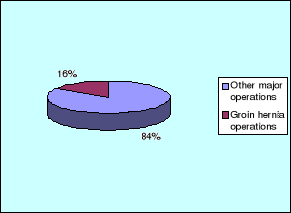
Figure 1 above shows the total of patients who underwent
major operations at Kibogora hospital in the period 18 months from 01/01/2007
to 30/06/2008 was 765 patients among them 121 were operated for groin hernias,
this made up a local hospital prevalence for groin hernia of 16%.
4.1.2. Socio-demographic
aspects
Figure 2: Distribution of patients basing on
Age
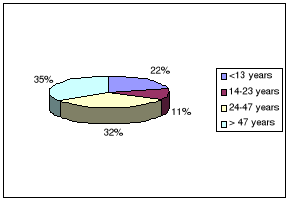
In our
study as it is demonstrated by figure 2 above, the majority of patients
42 (35%) was in the group of >47 years, followed by a group
of the age range 24-47 years with 39 (32%), < 13 years were 27(22%)
and came last the group of 14-23 years with 13 (11%),
the extremities were 1 year and 77 years.
Figure 3: Distribution of
patients basing on Sex
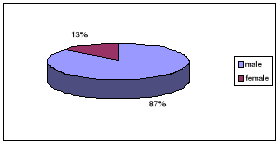
Figure 3 shows that the majority of our patients was male sex
making up 105 (87%). Only 16 (13%) of patients were female
Figure 4: Distribution of
patients basing on the mode of consultation
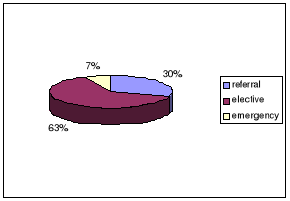
Figure 4 above shows that the biggest percentage of patients
under went elective surgery for hernia repair this making 77 (63%). Only 8
(7%) of all the patients were emergency. 36 (30%) were referred cases.
Figure 5: Distribution of
patients basing on the mode of their PMH
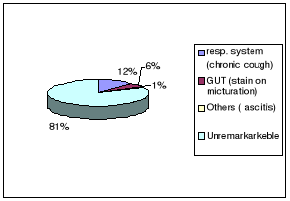
Figure 5 shows that 99 (81%) of the patients with groin hernia
had no remarkable previous medical status, 14 (12%) of the patients had
respiratory problems (as chronic cough), 7 (6%) of the patients had GUT
problems (as strain on micturation) and came last
(others such as ascitis) with only a 1%.
4.1.3. Clinical assessment
Figure 6: Distribution of
patients basing on the type of hernia
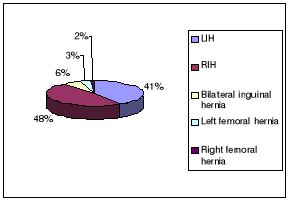
Figure 6 above demonstrates that most patients had inguinal
hernia i.e. 58 (48%) as RIH and 50 (41%) as LIH, 7 (6%) of the patients had
bilateral hernia. Femoral hernia was only seen in 5% of the patients (3%) as
left femoral hernia and 2 (2% as right femoral hernia)
Figure 7: Distribution of
patients basing on pre-operative diagnosis
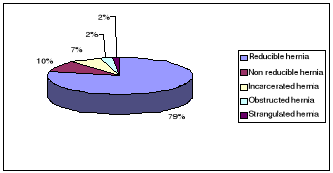
Figure 7 above demonstrates that the biggest percentage of the
patients in our study had reducible type of hernia and this constituted 95
(79%), followed by non reducible hernia with 12 (10%). Incarcerated hernia
hernia was 9 (7%), obstructed hernia and strangulated hernias had equal
percentages of 2 (2%) each.
Figure 8: Distribution of
patients basing on type of operation
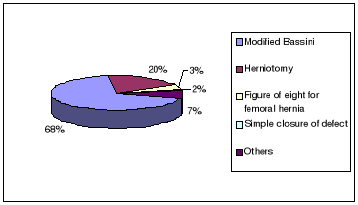
Figure 8 above shows Modified Bassini was the most type of
hernia repair performed constituting 83 (68%), this was followed by herniotomy
with a 24 (20%). Other nonspecified hernia repairs constituted 7%. Figure of
eight for femoral hernia repair constituted 3% and came last the simple closure
of defect with a 2%.
Figure 9: Distribution of
patients basing on anaesthesia
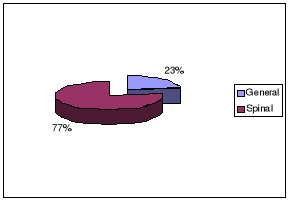
Figure 9 above shows that spinal anaesthesia was the mostly
used type of anaesthesia with 77% i.e. it was used in 93 hernia repairs out of
the 121 cases, only 28 (23%) of hernia repair were under general
anaesthesia.
Figure 10: Distribution of
patients basing on post-operative stay
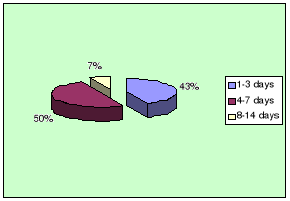
Figure 10 above indicates that 50% of the patients spent 4-7
days in the hospital postoperatively after hernia repair and this was the
highest percentage, 43% of the patients spent 1-3days post operatively and only
7% spent 8-14 days postoperatively. This indicates that the evolution of
patients' status after hernia repair was good.
Figure 11: Distribution of
patients basing on post-operative complications
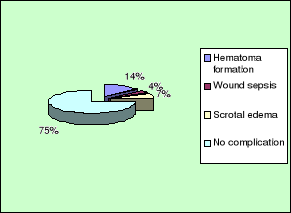
Figure 11 above demonstrates that most patients had no
complications after groin hernia repair and this constituted 91 (75%). Among
the complications seen after groin hernia repair in Kibogora hospital, wound
hematoma formation was the commonest with 17 cases making up (14%), scrotal
edema came second with 8 cases (7%) and wound sepsis was only in 5 cases making
only a 5%.
Figure 12: Distribution of
patients basing on condition on discharge
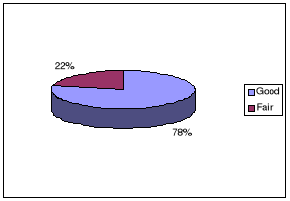
Figure 12 above demonstrates that the majority 94 (78%) of
patients were discharged in good condition, this is attributed to the advanced
surgical skills applied during hernia repair in Kibogora hospital, 22% of the
patients were discharged in fair condition. There was no death reported during
the study period.
4.1.4. Analytical results
Table 1: Distribution of
patients basing on comparing sex and type of groin hernia
|
SEX
|
TYPE OF GROIN HERNIA
|
TOTAL
|
P value
|
|
LIH
|
RIH
|
Bilateral inguinal hernia
|
Left femoral hernia
|
Right femoral hernia
|
|
|
|
Male
|
47 (38.8%)
|
52 (43%)
|
6
(5.0%)
|
0
(0%)
|
0
(0%)
|
105 (86.8%)
|
|
Female
|
3
(2.5%)
|
6 (5.0%)
|
1
(0.8%)
|
4
(3.3%)
|
2
(1.7%)
|
16 (13.2%)
|
|
Total
|
50 (41.3%)
|
58 (47.9%)
|
7
(5.8%)
|
4
(3.3%)
|
2
(1.7%)
|
121 (100%)
|
0.000 S
|
«S» for a p value means «significant»
Table 1 above shows that the majority of Groin hernia was
inguinal hernia and predominantly seen in male sex. Femoral hernia was only
seen in 6 cases and all cases were females.
Table 2: Distribution of
patients on comparing age range and type of Groin hernia
|
AGE RANGE
|
TYPE OF GROIN HERNIA
|
TOTAL
|
P value
|
|
LIH
|
RIH
|
Bilateral inguinal hernia
|
Left femoral hernia
|
Right femoral hernia
|
|
|
|
<13 years
|
10 (8.3%)
|
16 (13.2%)
|
1
(0.8%)
|
0
(0%)
|
0
(0%)
|
27 (22.3%)
|
|
14-23 years
|
6
(5%)
|
7 (5.8%0
|
0
(0%)
|
0
(0%)
|
0
(0%)
|
13 (10.7%)
|
|
24-47 years
|
19 (15.7%)
|
18 (14.9%)
|
1
(0.8%)
|
1
(0.8%)
|
0
(0%)
|
39 (32.2%)
|
|
> 47 years
|
15 (12.4%)
|
17 (14%)
|
5
(4.1%)
|
3
(2.5%)
|
2
(1.7%)
|
42 (34.7%)
|
|
TOTAL
|
50 (41.3%)
|
58 (47.9%)
|
7
(5.8%)
|
4
(3.3%)
|
2
(1.7%)
|
121 (110%)
|
0.317 NS
|
«NS» for a p value means «not
significant»
Table 2 above demonstrates that Groin hernia was predominantly
seen in the age range >
47 years although the difference was not statistically
significant (p value= 0.317). Inguinal hernias were the commonest type of groin
hernia seen.
Table 3: Distribution of
patients basing on comparing mode of consultation and Pre-operative
diagnosis
|
MODE OF CONSU-LTATION
|
PRE-OPERATIVE DIAGNOSIS
|
TOTAL
|
P value
|
|
Reducible
hernia
|
Non reducible hernia
|
Incarce-rated
hernia
|
Obstru-cted
hernia
|
Strang-ulated
hernia
|
|
|
|
Referral
|
25 (20.7%)
|
6
(5.0%)
|
5
(4.1%)
|
0
(0%)
|
0
(0%)
|
36 (29.8%)
|
|
Elective
|
70 (57.9%)
|
5
(4.1%)
|
2
(1.7%)
|
0
(0%)
|
0
(0%)
|
77 (63.6%)
|
|
Emergency
|
0
(0%)
|
1
(0.8%)
|
2
(1.7%)
|
3
(2.5%)
|
2
(1.7%)
|
8
(6.6%)
|
|
TOTAL
|
95 (78.5%)
|
12
(9.9%)
|
9
(7.4%)
|
3
(2.5%)
|
2
(1.7%)
|
121 (100%)
|
0.000 S
|
«S» for a p value means «significant»
Results in table 3 above: shows that the mode of consultation
differed from each type of pre-operative diagnosis, but all obstructed and
strangulated hernias were seen as emergency cases.
Table 4: Distribution of
patients basing on comparison between previous medical status and post
operative stay
|
PREVIOUS MEDICAL
STATUS
|
POST-OPERATIVE STAY
|
TOTAL
|
P value
|
|
1-3 days
|
4-7 days
|
8-14 days
|
|
Resp. system (chronic cough)
|
3 (2.5%)
|
9 (7.4%)
|
2 (1.7%)
|
14 (11.6%)
|
|
|
GUT (strain on micturation)
|
0 (0%)
|
5 (4.1%)
|
2 (1.7%)
|
7 (5.8%)
|
|
Others (ascitis)
|
0 (0%)
|
0 (0%)
|
1 (0.8%)
|
1 (0.8%)
|
|
Unremarkable
|
49 (40.5%)
|
47 (38.8%)
|
3 (2.5%)
|
99 (81%)
|
|
TOTAL
|
52 (43%)
|
61 (50.4%)
|
8 (6.6%)
|
121 (100%)
|
0.001 S
|
«S» for a p value means «significant»
Table 4 above shows a significant relationship (p=0.001)
between the previous medical status and the post-operative stay on the surgical
ward.
4.2. DISCUSSION
Here the results obtained in our study at Kibogora hospital
are compared with findings from other studies and we draft some conclusions and
recommendations.
A. Prevalence of Groin hernia
in Kibogora Hospital (Department of surgery)
At the end of our study we found
that the total of patients who underwent major surgical interventions in the
department of surgery at Kibogora Hospital from 01/01/2007 to 30/06/2008 i.e.
(in 18 months) was 765 patients of which 121 patients were operated for groin
hernia making a local hospital prevalence for GH 16%. Although the literature
does not prevail a reliable regional or international prevalence for GH, a
study carried out by Karuranga Ernest in March 2007 in Kanombe Military
Hospital came up with a prevalence of 14.7% in 59 cases recorded among a total
of 397 cases involved during the period of 12 months [8]. The
prevalence of Groin hernia is difficult to determine and the possible reasons
for this difficulty being; the inconsistency of data sources used and also lack
of standard differentiation of Groin hernia studies from abdominal wall hernia
in general.
B. Characteristics of patients
according to age
In total this study had a male population of 105 (87%) and
females at 16 (13%) and M: F ratio of 6.5:1. This shows a clear agreement with
the study conducted by Karuranga [8] which came up with a M: F ratio of 6.1:1.
Another study done by Kakande I and Odula P.O about Groin hernia in Mulago
Hospital Kampala also confirmed a male predominance [5]. The female
population in both studies was quite low. This may reflect the role of
increased abdominal pressure commonly seen in male sex especially with
advancing age.
C. Characteristics according to
clinical presentation and type/site of hernia
In Kibogora Hospital (Western province in Rwanda), most
patients 95/121 (79%) presented with uncomplicated reducible hernias, 2/121
(2%) presented as strangulated or obstructed hernias, others 12/121 (10%) and
9/121 (7%) presented as non reducible and incarcerated hernias. Basing on the
type/site of groin hernia our study revealed that most patients had inguinal
hernia i.e. 65/121 (54%), femoral hernia was only seen in 5% of all the cases.
Ohene-Yeboah [9] in Ghana reported that 71% of cases in his study
were inguinal hernias, 10% femoral hernias. In yet another study, by McConkey
[10] from Sierra Leone, had strangulated hernias representing 25% of
all emergency operations. Adesunkanmi in Nigeria, [11] in his study
of 250 consecutive patients, the incarceration rate was 25%, obstructed hernias
were said to represent 26% of all abdominal hernias.
D. Characteristics of patients
according to type of operation
In our study at Kibogora hospital we revealed a high tendency
to practising the Modified Bassini technique during hernia repair making up
68%. Other techniques included Herniotomy 20%, Non specifified repairs 7%,
figure of eight for femoral hernia repair at 3%, Simple closure of defect at
2%. Our study findings were very much consistent with various study findings.
In Karuranga's study at KMH in Kigali [8], Modified Bassini
technique took 52% of cases, followed by Herniotomy 15%. Comparatively to
another study by Odula and Kakande in Mulago Hospital, Kampala Uganda
[5], Modified Bassini technique constituted 68.2% of all cases,
Herniotomy at 16.9%, Simple closure of defect 1%. In all the above studies
Modified Bassini was the mostly employed technique during hernia repair.
E. Anaesthesia
This study at Kibogora Hospital showed a predominance of
applying Spinal anaesthesia during hernia repair with 77% of all hernia
repairs. The rest of cases were under General anaesthesia, no local anaesthesia
application was revealed during the study period. Elsewhere, in a study done in
northern Ghana by Wilhelm TJ et al [12], equally revealed that
spinal anesthesia was predominant with 48% ,followed by general anesthesia on
29.6% whilst local anesthesia on 22.4% which contrasts with our findings in
Kibogora hospital as regards the use of local anesthesia. This trend difference
can be explained by the fact that merits of local anesthesia use in elective
groin hernia repair in our settings are less known.
F. Post-operative
complications/ evolution
In our study, significant complications occurred in 30 (25%)
cases in a total of 121 cases which underwent groin hernia repair. Hematoma
formation was the most common post-operative complication encountered making up
17 (14%), scrotal edema came second with 8 (7%) and Wound sepsis came last with
only 5 (4%) cases. The majority of patients 94 (78%) was discharged from the
surgical ward in a good condition. Only 27 (22%) of were discharged in a fair
condition, no patient died during this study period. In another study by H Lau
and F. Lee in Hong Kong [14] to audit the outcome of 271 cases who
underwent inguinal hernia repair, no patient died, 265 (97%) cases were
discharged home on the day of operation and in good condition, wound
complication was the common morbidity encountered.
CHAPTER 5. CONCLUSION AND RECOMMENDATIONS
5.1. CONCLUSION
At the end of our study, we derived the following
conclusions:
1. The prevalence of GH at Kibogora Hospital was 16% in
121 cases recorded among
the 765 cases of major surgical interventions done
during the period of study.
2. There was a predominance of male sex as regards the
occurrence of GH in
Kibogora Hospital with a Male to Female ratio of
6:1.
3. Modified Bassini technique is the most commonly
performed procedure for Groin
Hernia repair in Kibogora Hospital.
4. Among the post-operative complications, hematoma
formation was predominant
with (14%), followed by scrotal edema at (7%) and
wound sepsis came last with
(5%).
5. The majority of patients who underwent hernia repair
at Kibogora Hospital
are discharged in good conditions.
6. Spinal anesthesia was mainly used during groin hernia
repair, this was followed by
General anesthesia and local anesthesia was not
applied at all during the study
period.
5.2. RECOMMENDATIONS
To the general population
Ø The entire population should all the time seek
medical help whenever they notice a swelling in the groin area because this
limits chance of developing complications.
To the Physicians
Ø General practitioners should always seek surgical
skills from senior surgeons on how to operate on the groin hernia in order to
minimise chances of patients developing post-operative complications.
To the hospitals
Ø Elective hernia repair should be encouraged in order
to prevent complications
Ø There is need for a prospective study on a wider
scale.
To the faculty of medicine, National University of
Rwanda (NUR)
Ø Improve training to enable students have rational
surgical knowledge to enable them improve their surgical skills in general but
more specifically for the management of hernias.
Ø Encourage more medical students to carry out research
on this subject in other hospitals and compare their results with our
findings.
To the ministry of health:
Ø The ministry should carry out a larger fully powered
study to determine the extent of this problem in all major hospitals in the
country and then take appropriate measures.
REFERENCES
1. Mann CV Hernias. Umbilicus. Abdominal wall In: Mann CV;
Russell RCG; Williams NS Bailey and Love's Short practice of surgery.
22nd ed. ELBS with Chapman and Hall, London 1995, Ch.55; 885-903.
2. Wantz GE Abdominal wall hernias In: Schwartz SI; Shires
GT; Spencer FC; Fischer JE Principles of surgery 7th ed. New York,
McGraw-Hill 1999, Ch.34; 1585-1612).
3. Zuckschwerdt W. Verlag , GmbH, Surgical treatment.
Abdominal wall. Hernias, pathogenesis 2001.
4. David C Brooks: Classification and diagnosis of groin
hernias; 16.2 May 27, 2008, www.Update.com.
5. Kakande I, Odula P 0, Groin Hernia in Mulago hospital,
Kampala. East and Central African Journal of Surgery Volume 9 Number 2 -
December 2004. 2004 - bioline. rg.br
6. Kark AE, Kurzer M, Waters KJ. Accuracy of clinical
diagnosis of direct and indirect inguinal hernia. Br J Surg 1994;
81:1081-1082.
[ISI]
[Medline]
7. Cameron AE. Accuracy of clinical diagnosis of direct and
indirect inguinal hernia. Br JSurg 1994; 81: 250.
[ISI][Medline.
8. Karuranga E., Prevalence and management of abdominal wall
hernia at Kanombe Miltary Hospital. From Jan 2006-jan 2007. A desertation
presented in partial fulfilments of the requirements for the award of MB.ChB.
of the national university of Rwanda.2007.
9. Ohene Yeboah M. Stangulated external hernias in Kumasi. W.
Africa J Med 200 22(4) : 310-31.
10. McConkey S.J. Case series of Acute Abdominal surgery in
rural Sierra Leone. World J. Surg 2002 26: 509-513
11. Adesunkanmi A.R Agbakwuru EA, Badmus T.A. Obstructed
Abdominal Hernia at the Wesley Guide Hosp, Nigeria. E Afr Med. J.2000 Jan 77(1)
: 31-33.
12. Wilhelm TJ, S,Anemana , P. KyamanywA, J. Rennie , S. Post
, S.Freudenberg . Anaesthesia for elective inguinal hernia repair in rural
Ghana, Appeal for local anaesthesia in resource-poor countries. (2006 The Royal
Society of Medicine Press). Tropical Doctor, Volume 36, N° 3, Pp
147-149.
13. Paola Primatesta and Micheal J. Goldacre. Inguinal Hernia
Repair: Incidence of Elective and Emergency Surgery, Readmissions and
Mortality. International Journal of Epidemiology. Volume 25, Number-4, pp.
835-839. (1996 Oxford University Press).
14. Lau H, Lee H , An audit of the early outcome of ambulatory
inguinal hernia at a surgical day-care centre. Day Surgery Centre, Department
of Surgery, The University of Hong Kong Medical Centre, Tung Wah Hospital,
Sheung Wan, Hong. 218 HKMJ Vol 6, No 2 June 2000.
15. Ramyil V.M, Iya D, Ogbonna B.C, Dakum N.K. Safety day care
hernia repair in Jos, Nigeria. East African Medical Journal ISSN 0012-835X.
(2000, Vol.77, No 6, pp. 326-328).
APPENDIX
DATA COLLECTION SHEET
|
No
|
Descriptive question
|
Response
|
Code
|
|
REGISTRATION DATA
|
|
1
|
Age
|
< 13 years
|
1
|
|
14-3 years
|
2
|
|
24-46 years
|
3
|
|
> 47 years
|
4
|
|
2
|
Sex
|
Male
|
1
|
|
Female
|
2
|
|
3
|
Mode of consultation
|
Referral
|
1
|
|
Elective
|
2
|
|
Emergency
|
3
|
|
4
|
Previous Medical Status
|
Resp. system (e.g. Chronic cough)
|
1
|
|
GIT ( e.g. constipation)
|
2
|
|
GUT (e.g. strain on micturation)
|
3
|
|
Obstetrical (pregnancy)
|
4
|
|
Others ( e.g. ascitis)
|
5
|
|
Unremarkable
|
6
|
|
CLINICAL ASSESSMENT
|
|
5
|
Site/type of Groin Hernia
|
LIH
|
1
|
|
RIH
|
2
|
|
Bilateral Inguinal Hernia
|
3
|
|
Left Femoral Hernia
|
4
|
|
Right Femoral Hernia
|
5
|
|
6
|
Pre-operative diagnosis
|
Reducible Hernia
|
1
|
|
Non reducible
|
2
|
|
Incarcerated Hernia
|
3
|
|
Obstructed Hernia
|
4
|
|
Strangulated Hernia
|
5
|
|
7
|
Type of operation
|
Modified Bassini technique
|
1
|
|
Shouldice
|
2
|
|
Herniotomy
|
3
|
|
Figure of eight for Femoral hernia
|
4
|
|
Simple closure of defect
|
5
|
|
Others
|
6
|
|
8
|
Anaesthesia
|
General anaesthesia
|
1
|
|
Spinal anaesthesia
|
2
|
|
Local anaesthesia
|
3
|
|
9
|
Post-operative stay (in days)
|
1-3 days
|
1
|
|
4-7 days
|
2
|
|
8-14 days
|
3
|
|
> 2 weeks
|
4
|
|
10
|
Post-operative complications
|
Hematoma formation
|
1
|
|
Retension of urine
|
2
|
|
Wound sepsis
|
3
|
|
Wound sinus
|
4
|
|
Testicular ischemia
|
5
|
|
Nerve entrapment
|
6
|
|
Scrotal edema
|
7
|
|
11
|
Condition on discharge
|
Good condition
|
1
|
|
Fair condition
|
2
|
|
Died
|
3
|
| 

