|
SERVICE QUALITY AT A MILITARY HOSPITAL
BY
PONCE
KOKOU
MINOR DISSERTATION
Submitted in partial fulfilment of the
requirements for the degree
MAGISTER COMMERCII
in
BUSINESS MANAGEMENT
in
the
FACULTY OF MANAGEMENT
at the
UNIVERSITY OF
JOHANNESBURG
Supervisor: Prof Mornay Roberts-Lombard
JANUARY 2014
Co-supervisor: Dr Estelle van Tonder
ii
ABSTRACT
With the raise of competition in the Gabonese health industry
and increased costs, most health service providers in Gabon have become under
pressure to deliver good service quality. This also relates to the military
hospital in Libreville in Gabon striving to provide adequate health services to
its patients. The cost for hospitals to attract patients through several means
such as providing good service quality has become crucial. Patient loyalty and
retention can have an important financial advantage for a hospital, thus it has
become essential for hospitals to create a sustaining relationship with their
patients. The question of assessing service quality presents itself. This study
investigated service quality at a military hospital in Libreville in Gabon. It
was the objective of this study to establish if there is a difference in how
patients rate doctors and nurses on the service quality dimensions.
This research was quantitative and descriptive in nature.
Theory relating to service quality and patient satisfaction was provided. The
population for the study consisted of patients who were at least 18 years old,
males and females, who have experienced medical services and stayed over at the
military hospital for at least one night. A self-administered questionnaire was
designed based on the theoretical literature illustrated in the study. The
questionnaire assessed various elements that were identified through the
literature review. The questionnaire was based on a set of statements linked to
the literature theory, and a 7-point Likert scale which enabled respondents to
choose from seven different alternatives ranging from strongly disagree to
strongly agree. A number of statistical analysis techniques were undertaken to
achieve the objectives of the study, such as factor analysis. The conclusion
and findings of the research assisted in explaining the objectives of the study
and the results of the statistical analysis were found to reject the hypotheses
that there is no significant difference in how patients rate the reliability,
responsiveness, assurance and empathy of doctors and nurses and to reject the
hypothesis that patients do not have a positive perception of the tangible
aspects of a military hospital in Libreville, Gabon.In terms of the doctors'
services, patients felt a need for more privacy in terms of the confidentiality
of their treatment, a need for more individual attention, a need to be heard,
and to trust doctors. Therefore such needs could be addressed through improved
compassion, communication and understanding of doctors during the diagnosis of
the problem. The feeling expressed was that doctors should pay more attention
to patients' problems and share with them
iii
their experience. Doctors at the military hospital should
develop more work ethic where patients' records and cases should never be
discussed with anyone without patients' permission. The military hospital
should employ highly trained and qualified doctors to address the trust issue
with patients. Lastly, consultation time may need to be reviewed to add some
extra time to better address patients' needs during their consultation with
doctors.
In terms of the services delivered by nurses towards patients,
the latter were of the opinion that there was a need for more individual
attention from nurses. Such individual attention could include greater
information sharing when a patient is treated, friendlier communication to
install greater trust and respect. Such needs could be addressed through
improved patience, compassion and understanding by nurses during their dealings
with patients. Nurses should also develop more work ethic regarding patients'
records, and cases should never be discussed with anyone without their
permission. Officials in the hospital should hire highly trained and qualified
nurses to address the issue of trust in patients and consultation time may need
to be reviewed to add some extra time to better address patients' needs during
their dealings with nurses.
iv
DECLARATION
I, the undersigned Ponce Kokou, hereby declare that this
dissertation is my own original work. It has not been presented or submitted
before for any degree at this or at any other university. Any assistance
received in preparing this work has been duly acknowledged in this
dissertation. It is submitted in fulfilment of the requirements for the degree
of Master of Commerce in Business Management at the University of
Johannesburg.
Signature (Day, month, year)
v
ACKNOWLEDGEMENTS
First, I thank the almighty God, Jesus Christ, for giving me his
love, strength, wisdom, courage, determination and inspiration, without which I
would never been able to complete this work.
Also, I would like to thank the following people for their
involvement to this dissertation:
? My mother and father, Adèle and Paul Kokou in Gabon
for their continued love, support and encouragement, during this tough journey.
I pray to the Lord Jesus Christ to continue blessing you and to give you many
more years and reward you in abundance. Your presence in my life is all I ever
wanted. Merci Papa Paul et Madre pour tout le soutien, l'amour, la
tendresse, l'affection et la confiance dont vous m'aviez toujours
apporté. Je ne pourrai jamais vous remercier assez. Que le Seigneur
Jésus Christ, Dieu tout puissant vous accorde protection, santé,
paix, et très longue vie. Sans vous, je n'aurai jamais achevé ce
diplôme, vous êtes ma vie, mon coeur, vous représentez tout
pour moi.
? My brothers and sisters Nicaise, Ghislaine, Alain, Wilfried,
Maryse, Marina, Nancy, nieces and nephews Fatoumata, Bertrand, Nanou, Celia,
Ruby, Sarah for their continued support, prayers, love and guidance during this
difficult journey. I pray to the Lord Jesus Christ to continue blessing you and
giving you many more years. Thank you for believing in me.
? My supervisors Prof Mornay Roberts-Lombard and Dr Estelle
Van Tonder as well as Richard Devey from STATKON for their continued advice,
guidance and patience. Thank you for assisting me in overcoming the challenges
experienced during this long journey. The road was tough, but you drove me
through it. May God almighty bless and reward you abundantly.
vi
DEDICATION
To the Lord Jesus Christ, to the much-loved family in the
world, Mr and Ms Kokou, my brothers, sisters, nephews and nieces.
vii
TABLE OF CONTENTS
ABSTRACT ii
DECLARATION iv
ACKNOWLEDGEMENTS v
DEDICATION vi
TABLE OF CONTENTS vii
LIST OF TABLES xii
LIST OF FIGURES xiv
CHAPTER 1 : CONTEXTUALISATION OF THE STUDY
1
1.1 INTRODUCTION 1
1.2 BACKGROUND 2
1.3 PROBLEM STATEMENT 4
1.4 PURPOSE OF THE STUDY 4
1.5 OBJECTIVES 5
1.5.1 Primary objective 5
1.5.2 Secondary objectives 5
1.5.3 Hypotheses 5
1.6 SIGNIFICANCE OF THE STUDY 6
1.7 LITERATURE REVIEW 6
1.7.1 Overview of the service sector 6
1.7.2 Service marketing in health care organisations
7
1.7.3 Service quality 8
1.7.4 Service quality and patient satisfaction
8
1.7.5 Measuring service quality using the SERVQUAL
instrument 9
1.8 RESEARCH METHODOLOGY 11
1.9 ETHICAL CONSIDERATIONS 13
1.10 LIMITATIONS OF THE STUDY 13
1.11 DIVISION OF THE STUDY 14
1.12 TERMINOLOGY 15
1.13 CONCLUSION 17
VIII
CHAPTER TWO: THE HEALTH CARE INDUSTRY IN AFRICA AND
GABON
|
19
|
|
2.1
|
INTRODUCTION
|
19
|
|
2.2
|
HEALTH CARE STATUS IN AFRICA
|
19
|
|
2.3
|
HEALTH DEVELOPMENT INITIATIVES IN CENTRAL AFRICA
|
21
|
|
2.4
|
HEALTH SERVICE QUALITY IN GABON
|
23
|
|
2.4.1
|
Public health development initiatives in Gabon
|
23
|
|
2.4.2
|
Private sector development initiatives in Gabon
|
24
|
|
2.5
|
IMPLICATIONS OF HEALTH SERVICE QUALITY IN GABON
|
27
|
|
2.6
|
HEALTH DEVELOPMENT INITIATIVES IN GABON
|
27
|
|
2.7
|
THE MILITARY HOSPITAL IN GABON
|
30
|
|
2.6
|
CONCLUSION
|
36
|
CHAPTER THREE: SERVICES MARKETING, SERVICE QUALITY AND
CUSTOMER
|
SATISFACTION
|
38
|
|
3.1
|
INTRODUCTION
|
38
|
|
3.2.
|
SERVICES MARKETING
|
40
|
|
3.2.1
|
Definition of services marketing
|
40
|
|
3.2.2
|
Generic elements of the definition of services marketing
|
42
|
|
3.2.3
|
The importance of services marketing
|
44
|
|
3.3
|
MANAGING ORGANISATIONS IN A SERVICE ENVIRONMENT
|
47
|
|
3.3.1
|
Different dimensions when managing an organisation in a
service
|
|
|
environment
|
47
|
|
3.3.2
|
The services marketing mix
|
49
|
|
3.4
|
THE THREE LEGS OF SERVICES MARKETING
|
52
|
|
3.4.1
|
The services marketing triangle
|
52
|
|
3.5
|
SERVICE QUALITY
|
54
|
|
3.5.1
|
Defining service quality
|
55
|
|
3.5.2
|
Generic elements of service quality
|
56
|
|
3.5.3
|
The importance of service quality
|
57
|
|
3.5.4
|
The different elements of service quality
|
58
|
|
3.5.5
|
Failure gaps in service quality
|
59
|
|
3.6
|
CUSTOMER SATISFACTION
|
62
|
|
3.6.1
|
Defining customer satisfaction
|
62
|
|
3.6.2
|
Satisfaction with care between doctors and nurses
|
63
|
|
3.6.3
|
The generic elements to customer satisfaction
|
64
|
|
3.6.4
|
Types of customer expectations and the zone of tolerance
|
65
|
|
3.6.5
|
Factors influencing service expectations
|
66
|
ix
3.6.5.1 Desired and predicted service 66
3.6.5.2 Adequate service 67
3.6.6 The link between expectations, customer
satisfaction and service
quality 68
3.7 CONCLUSION 69
CHAPTER FOUR: RESEARCH METHODOLOGY 71
4.1 INTRODUCTION 71
4.2 THE RESEARCH PROCESS 71
4.2.1 Step 1: Identify and formulate the problem or
opportunity 72
4.2.2 Step 2: Determine the research objectives
73
4.2.3 Step 3: Research design 73
4.2.3.1 Quantitative research 74
4.2.3.2 Descriptive research 74
4.2.4 Step 4: Conduct secondary research
75
4.2.5 Step 5: Select a primary research method
75
4.2.5.1 Data gathering technique 75
4.2.5.2 Self-administered questionnaires
76
4.2.5.3 Covering letter 77
4.2.5.4 Questionnaire 77
4.2.5.5 Questionnaire design 78
4.2.5.6 Pretesting of the questionnaire 83
4.2.5.7 Reliability and validity of the questionnaire
84
4.2.6 Step 6: Determine the research frame
86
4.2.6.1 The survey area 86
4.2.6.2 The study unit 86
4.2.6.3 Population 86
4.2.6.4 Sampling method 87
4.2.6.5 Probability sampling method 88
4.2.6.6 Sample technique 88
4.2.6.7 Sample size 90
4.2.7 Step 7: Data gathering 92
4.2.8 Step 8: Data analysis 92
4.2.8.1 Editing of data 93
4.2.8.2 Coding of data 93
4.2.8.3 Processing and statistical analysis of data
94
4.3 RALIABILITY OF THE RESULTS 95
4.3.1 Sampling errors 95
X
4.3.2 Response errors 95
4.3.3 Non-response errors 95
4.4 CONCLUSION 96
CHAPTER FIVE: DATA ANALYSIS AND INTERPRETATION
97
5.1 INTRODUCTION 97
5.2 MEASUREMENT OF OBJECTIVES AND HYPOTHESES
97
5.3 RESEARCH INSTRUMENT AND RESPONSE STATISTICS
98
5.4 DISCUSSION OF THE RESEARCH FINDINGS 99
5.4.1 Section A - Demographics 99
5.4.2 Section B: Perception of services provided by doctors
and nurses ... 103
5.4.2.1 Patient perception of services provided by
doctors and nurses 103
5.4.2.2 Comparing patient perception of services
delivered by doctors and
nurses 112
5.4.3 Section C: Perceptions of patients towards the
tangibility dimension of
the hospital 115
5.4.4 Section D: Overall perception of services
117
5.4.5 Section E: Factors that could influence the choice for
the military
hospital 119
5.5 ACCEPTANCE OR REJECTION OF HYPOHESES
121
5.6 MEASUREMENT OF THE OBJECTIVES 122
5.7 CONCLUSION 123
CHAPTER SIX: CONCLUSIONS, IMPLICATIONS AND
RECOMMENDATIONS 125
6.1 INTRODUCTION 125
6.2 MAIN CONCLUSIONS, IMPLICATIONS AND RECOMMENDATIONS
OF THE STUDY 125
6.2.1 Perceptions of patients regarding the four service
quality dimensions
investigated in this study 126
6.3 PATIENTS' PERCEPTIONS REGARDING THE TANGIBLE ASPECTS
AT A SPECIFIC MILITARY HOSPITAL 131
6.4 OVERALL PERCEPTION OF SERVICES AND FACTORS THAT
COULD INFLUENCE THE CHOICE OF A MILITARY HOSPITAL
132
6.5 LIMITATIONS OF THIS STUDY 133
6.5.1 Limitations based on the literature review
133
6.5.2 Limitations of the empirical phase of study
134
6.6 RECOMMENDATIONS FOR FUTURE RESEARCH
134
6.7 CONCLUDING REMARKS 134
xi
REFERENCES 135
APPENDIX A: COVERING LETTER 150
APPENDIX B: QUESTIONNAIRE 151
APPENDIX C: CONFIRMATION OF LANGUAGE EDITING
157
xii
LIST OF TABLES
TABLE 2.1: Department of emergency 30
TABLE 2.2: Department of medical analysis 31
TABLE 2.3: A pharmacy 32
TABLE 2.4: Department of inernal mecicine 33
TABLE 2.5: Department of surgery and orthopaedic 33
TABLE 2.6: Department of ophthalmoloty 34
TABLE 2.7: Department of Ear, Nose and Throat (ENT) 34
TABLE 2.8: Department of radiology 35
TABLE 2.9: Military hospital 35
TABLE 3.1: Definition of services marketing 41
TABLE 3.2: Definition of service quality 55
TABLE 3.3: Definition of customer satisfaction 62
TABLE 4.1: Reliability statistics (Doctors and Nurses) 85
TABLE 4.2: Minimum sample size estimates 91
TABLE 5.1: Respondents' approaches and response rate 98
TABLE 5.2: Frequency of selected demographic variables of the
sample 99
TABLE 5.3: Frequency of the number of visits to the hospital and
duration of the visit 102
TABLE 5.4: Patients' perception of doctors' reliability 103
TABLE 5.5: Patients' perception of nurses' reliability 105
TABLE 5.6: Patients' perception of doctors' responsiveness 106
TABLE 5.7: Patients' perception of nurses' responsiveness 107
TABLE 5.8: Patients' perception of doctors' assurance 108
TABLE 5.9: Patients' perception of nurses' assurance 109
TABLE 5.10: Patients' perception of doctors' empathy 110
TABLE 5.11: Patients' perception of nurses' empathy 111
TABLE 5.12: Overall means scores, standard deviations and p-value
for the
reliability of doctors and nurses 113
TABLE 5.13: Overall
means scores, standard deviations and p-value for the
responsiveness of doctors and nurses 114
TABLE 5.14: Overall
means scores, standard deviations and p-values for the
assurance of doctors and nurses 114
TABLE 5.15: Overall
means scores, standard deviations and p-values for the
empathy of doctors and nurses 115
xiii
TABLE 5.16: Tangible aspects 116
TABLE 5.17: Overall means sc ores and standard deviations for
the tangibility
dimensions of service quality as rated by the respondents
117
TABLE 5.18: Overall perception of services 117
TABLE 5.19: Overall means score and standard deviation for the
overall perception
of service delivery as rated by the respondents 118
TABLE 5.20: Influential factors 119
xiv
LIST OF FIGURES
FIGURE 3.1: The services marketing triangle 52
FIGURE 3.2: Service quality gap model 60
FIGURE 4.1: Stages in the research process 71
FIGURE 4.2: Target population, sample units, sample elements
and actual
sample size 86
1
CHAPTER 1 : CONTEXTUALISATION OF THE STUDY
1.1 INTRODUCTION
Service quality refers to the ability of a product or a
service to satisfy customers' needs. The quality of service provided by an
organisation is crucial in the way it can determine the competitiveness of an
organisation (Vanniarajan, 2010:1). Service quality and customer satisfaction
are two correlated concepts in the services industry and service quality can
influence significantly on customers' satisfaction. Customer satisfaction
results from the difference between customers' expectations of services and the
actual service performance. A customer is satisfied if services match or go
beyond his or her expectations and is dissatisfied if service quality does not
meet his or her expectations (Naik, 2010:240).
Customer satisfaction is often operationalised by asking
customers about their general satisfaction level with services received
(Olusoji, 2009:6). In the medical industry, the World Health Organisation
policy states that everyone should have the right to enjoy the highest standard
of health service quality without any race, religious, political belief,
economic or social distinction (WHO, 2007).Patients' views on service quality
are vital to enhance superior services that meet their expectations (Olusoji,
2009:17). Unfortunately, individuals seeking medical services in hospitals in
Gabon have often been passively receiving health care service. Their views on
how they regard service quality have often been disregarded. The health care
system in Gabon is mainly provided by the government. As a result, most of the
hospitals in the country are mainly public or government hospitals. There are
however also private institutions that offer medical services to the
population. The majority of the hospitals are located in the main capital city
of Libreville where diseases such as tuberculosis, malaria, sleeping disorders,
and leprosy can be cured. However, health care services are often inadequate
and lacking in other parts of the country. As a result, patients often travel
to the main capital to seek better medical care (Health and Safety in Gabon,
2011).
The military hospital in Gabon in contrast, appears to attract
and provide good service quality to patients. It is a military owned medical
institution, located in the main capital of Libreville. Since its inauguration
in 2005, there has been an increased number of patients patronised by the newly
established medical care services. The hospital is
2
equipped with high-tech medical equipment, and managed by a
range of qualified medical staff such as general practitioners, specialists,
surgeons and nurses. The military hospital has been delivering quality services
to the population and attracted lots of patients in recent years (Hôpital
d' instructions des armées, 2011).Given the fact that the military
hospital in Gabon has been attracting more patients, the study will be
comparing the views of patients regarding the service delivery by doctors and
nurses at the military hospital in Libreville in Gabon. It is worth to
establish a comparison of the service delivery by doctors and nurses, since the
investigation may help executives at hospitals as well as at government level
to assess and address aspects related to satisfaction or dissatisfaction of
patients. In addition, the research intends to promote strategies to enhance
satisfaction and services performance in health care systems (Mekoth et al.,
2012:16).
This chapter comprises of a background to the research
followed by the problem statement and a theoretical overview of the service
sector, services marketing in health care, service quality, as well as a view
on SERVQUAL as an instrument to measure service quality and patient
satisfaction. A literature on research methodology will appear at the end of
the chapter.
1.2 BACKGROUND
Gabon has one of the most desirable medical services in
central and West Africa. The State is perceived as the main supplier of health
services in the country. As a result, most of the medical institutions in the
country are owned by the State. There are also private institutions that offer
medical services to the inhabitants. There have been a growing number of
medical facilities in the region from 1985 to present with the number of
medical facilities having increased from 28 in 1985 to 87. In addition, 312
dispensaries and infirmaries were also created. There are 29 medical doctors
available for every 100 000 individuals. 90% of the population of Gabon can
access medical services offered by the state in contrast to the remaining 10%
of the citizens who access medical services offered by private institutions
(Health and Safety in Gabon, 2011). Among the 90% of the people who access
government hospitals, only 21% can have proper medical services. 69% of the
remaining patients are receiving poor or inadequate health care. Most hospitals
are located in the main capital city of Libreville
3
where sicknesses like tuberculosis, malaria, sleeping
disorders, and leprosy can be treated. However, health care services are often
inadequate and lacking in other regions in the country. As a result, patients
often travel to the main capital to seek better medical care (Health and Safety
in Gabon, 2011).The US Department of State Travel Advisory (2010) observed that
most of the medical facilities in Gabon still remain limited in terms of proper
infrastructures, sanitation, medical practices, qualified medical staff and
technology. However, these facilities are in general good for daily routine or
the basic needs of the population. Most of the population of Gabon remain
concentrated in the main city of Libreville where they can easily access
medical treatments (Proquest, 2007:1).
The military hospital has been operating since 2005. The
facility is situated in Libreville and has been reputed for attracting lots of
patients in the region (Hôpital d' instructions des armées,
2011).This phenomenon has raised concerns of why patients have been massively
attracted to the military hospital. Should hospitals in Gabon understand the
needs of their patients and provide service quality to them, it could be
possible to increase their number of patients. Service quality in health care
is fundamental for satisfying patients, keeping them and making them loyal
(Naik, 2010:239).The importance of service quality should not be neglected.
There is a strong relationship between service quality, patient satisfaction
and profit. Patients, who are satisfied with services, are more likely to
communicate their satisfaction to friends and family. As a result, this can
attract a large number of customers and lead to increasing return. Patients
often praise hospitals that offer service quality that meets or exceeds their
expectations, and they are dissatisfied by those that provide inferior services
and patients are more likely to seek medical services that offer better
services (Naik, 2010:242).
The military hospital in Libreville in Gabon seems to be a
good example of investigation since it has increased its market share in the
health care industry in Gabon. Hence, it could be worthwhile to compare the
views of patients regarding the service delivery by doctors and nurses at the
military hospital in Gabon in order to determine strategies that could be
recommended to the other hospitals in the country to improve their service
quality and enhance patient satisfaction.
4
1.3 PROBLEM STATEMENT
The government of Gabon has improved the health care system in
the country through the provision of health care infrastructures, and by
increasing the number of government hospitals in the country in order to allow
more patients to have access to medical care services. However, the military
hospital seems to have increased its market share in the health industry. The
new hospital has attracted a large number of patients from various parts of the
country. There is no clear understanding of why patients have been attracted to
the military hospital. During a telephone interview conducted on 6 March 2012,
a medical personnel at the military hospital stated that patients seem to have
been satisfied with service quality provided in the military hospitals.
Moreover, the link between services delivery between doctors and nurses at the
military hospital in Gabon and patient satisfaction has not been yet
investigated before; hence these two features need to be investigated as the
study could offer a way to promoting effectiveness and profitability in medical
institutions.
1.4 PURPOSE OF THE STUDY
In health care, service quality can lead to patient
satisfaction or dissatisfaction. (Olusoji, 2009:7). Superior services provided
in hospitals often result in high levels of satisfaction. Satisfied patients
with services are more likely to repeat purchases, to remain loyal and to
follow the medical recommendations. In addition, it is worth investigating
service quality and patient satisfaction as it can enhance policies to improve
services delivery in hospitals (Olusoji, 2009:16-17). Given the importance of
service quality and customer satisfaction, the purpose of the study was to
assess the service quality of doctors and nurses at a military hospital located
in the city of Libreville in Gabon. The investigation attempted to determine if
there is a difference in how patients rate doctors and nurses on the service
quality dimensions. Insight into these findings could assist in determining
whether doctors and nurses varied significantly in terms of their level of
contribution to each service quality dimension, and which one of the groups
subsequently played the greatest role in the overall service quality provided
by the hospital. The study makes a contribution to the medical care industry
and the analysis of the empirical data will assist in determining strategies
that could be recommended to the other hospitals in Gabon to improve their
service quality and enhance their customer satisfaction.
5
1.5 OBJECTIVES
1.5.1 Primary objective
To establish the perceptions of patients regarding the service
quality received from doctors and nurses. More particularly, how they rate
doctors and nurses on the service quality dimensions.
1.5.2 Secondary objectives
· To determine how patients rate the reliability
of doctors and nurses.
· To establish how patients rate the responsiveness
of doctors and nurses.
· To determine how patients rate the assurance of
doctors and nurses.
· To establish how patients rate the empathy of
doctors and nurses.
· To establish if there is a difference in how patients
rate doctors and nurses on the service quality dimensions.
· To establish the perception of patients regarding the
tangible aspects of a military hospital in Gabon.
1.5.3 Hypotheses
The hypotheses below result from the above objectives:
H01: There is no significant difference in how patients rate the
reliability of doctors and nurses.
HA1: There is a significant difference in how patients rate the
reliability of doctors and nurses.
H02: There is no significant difference in how patients rate the
responsiveness of doctors and nurses.
HA2: There is a significant difference in how patients rate the
responsiveness of doctors and nurses.
H03: There is no significant difference in how patients rate the
assurance of doctors and nurses.
6
HA3: There is a significant difference in how patients rate
the assurance of doctors and nurses.
H04: There is no significant difference in how patients rate
the empathy of doctors and nurses.
HA4: There is a significant difference in how patients rate
the empathy of doctors and nurses.
H05: Patients do not have a positive perception of the
tangible aspects of a military hospital in Libreville, Gabon.
HA5: Patients do have a positive perception of the tangible
aspects of a military hospital in Libreville, Gabon.
1.6 SIGNIFICANCE OF THE STUDY
This research takes place in Libreville, in Gabon. This study
is immensely significant in various ways to the health care industry,
management, and to policy makers in Gabon. Assessing how patients perceive
service quality between doctors and nurses in a hospital in Gabon has never
been conducted before. The findings and result of this research will highlight
a more reliable scientific evaluation of the level of patient satisfaction with
service quality provided by doctors and nurses. The study will mainly reveal
dimensions of service quality between doctors and nurses that patients believe
important. This will offer empirical support for management's strategic
decisions in various key areas of their functions.
1.7 LITERATURE REVIEW
1.7.1 Overview of the service sector
The service sector is that section of economic activities
that provides intangible goods. It can range from communication, insurance,
administrative, electricity generation, banking, retail trades and health care
services. Unlike the manufacturing sector, the service sector employs intensive
human capital rather than natural capital (Fernandes, 2009:469). In the modern
economy, the service sector has grown considerably
7
compared to other sectors in the world economy. Over two
thirds of economic activities in the globe are comprised of services. In
European and Asian countries, service sector has considerably increased. The
sector encompasses more labour force than any other sector, and this has led to
economic growth and a decrease in the poverty level (World Bank, 2006:6).
The World Bank (2008:2) report shows a positive relationship
between efficiency in services and economic expansion in most parts of the
world. Increasing activities in the
service sector have progressively led to enhancing aggregate
productivity and
efficiency of other sectors in most countries'
economies.
1.7.2 Service marketing in health care
organisations
Service marketing in the hospital industry refers to the
planning, implementation and control of medical services delivery designed to
target patients' needs through the use of an effective, price conscious,
communication and distribution strategy (Dosen, 2009:205). Services marketing
has become the focus point of most health care organisations and hospitals are
willing to invest in service marketing. Services that meet patients'
expectations often result in a positive word-of-mouth, patient loyalty,
hospital profitability and patient satisfaction with medical care (Olusoji,
2009:7).The importance of sustaining a marketing strategy in hospitals has
arisen from the rise of rivalry, when there is a growing number of medical
institutions in the same region or when resources and customers become scarce,
for instance. Another driving force to sustain a marketing strategy is where
hospitals spending on services exceed their limited financial support (Dosen,
2009:206).
Because of the limited financial resources in both private
and public hospitals, health care executives have ventured to be more
interested in services marketing. Services marketing can promote effective
partnership between all the associates in the medical network such as patients,
potential associates, medical staff and executives. This aspect is vital to the
success of an organisation (Zainuddin, Previte & Russell-Bennett,
2011:364). In addition, health care services result from a high level of
interactions between medical staff and patients. Therefore, medical
professionals should exercise services marketing know-how and their expertise
to effectively inform patients and
8
address their health concerns. This is critical to enhance
service quality in health care (Dosen, 2009:206).
Furthermore, patients in the new millennium are well informed
about services quality; this has resulted from the expansion of the Internet.
Patients can today review, evaluate and compare services from one service
provider to another. Hospitals are currently required to improve their services
marketing in order to remain competitive (Dosen, 2009:207).
1.7.3 Service quality
Service quality is a complex approach due to its intangible,
heterogenic, inseparable and perishable characteristic. Measuring service
quality should be closely associated with the user's perceptions and
expectations of services provided (Naik, 2010).In health care settings, quality
care that meets patient expectations will often lead to satisfaction compared
to those that do not (Al Sharif, 2008:2).
Achieving service quality has become a central vision in most
health care organisations, since superior services can lead to patient loyalty
and retention (Olusoji, 2009:7). Services marketing has become a new tool as it
can significantly influence the behaviour of health care services users and
improve service quality provided in hospitals (Revere, 2010:39). Most hospitals
use the Internet as a services marketing tool for instance to market their
services to patients. The latter usually access the Internet to have
information about the type of service provided in health care (Revere,
2010:39).The Internet can enable interactions between services providers and
patients, who regularly assess and compare quality care in hospitals. Patients
can post, suggest or rate service quality performance via the Internet. This
has led hospitals to capitalise patients' views and expectations on medical
services and to improve quality (Revere, 2010:40).
1.7.4 Service quality and patient
satisfaction
Services quality is strongly correlated to patient
satisfaction in health care. Superior services often lead to a high degree of
patient satisfaction, patients' retention and loyalty (Olusoji, 2009:7). As a
result, a positive word-of-mouth is observed as patients will refer the medical
facility to friends and family (Kyle, 2010:3).
9
Kim (2008:6) explained in his research on childbirth that a
decline in service quality experienced by women after childbirth in Home Health
Agency in the United States, led to a decline in women satisfaction with
services provided. This study confirms that the level of services provided in
medical care is a predecessor of satisfaction or dissatisfaction. As a result,
patient satisfaction with services is regarded as a fundamental condition to
adherence and fidelity. Another study showed that patients value services in
health care more on functional quality, instead of on technical quality
(Yesilada & Direktor, 2010: 963). Technical quality relates to the
precision of the medical process that leads to cure, while functional quality
refers to the way medical services are administered to patients, such as care.
This leads patients to value more interpersonal relationships with medical
staff. Functional quality is seen to be positively linked to patients'
satisfaction or dissatisfaction with services provided in health care. In this
regard, patients often rely more on attitudes such as `care' of the service
provider as an indicator of service quality, rather than the `curing
performance' in health care (Mekoth et al., 2012: 17-18).
Thus, care is regarded to be positively linked to patient
satisfaction. Medical doctors often concentrate on providing the correct
treatment to patients and they think this is the main concern of patients. As a
result, patients' views of services quality may deviate from the services
providers'. This may lead to patients' dissatisfaction with services provided,
as the latter may usually require more attention and care from physicians
(Yesilada & Direktor, 2010: 963).
1.7.5 Measuring service quality using the SERVQUAL
instrument
Service delivery in health care has significantly improved in
recent years. Competition among health care service providers has forced
medical services to review their service delivery systems. Health care policies
have shifted towards providing services that satisfy the needs and desires of
patients. This new approach emphasises the views and needs of patients in
contrast to the former approach that focused on preferences and decisions of
medical employees (Desai, 2011: 40).Various studies have indicated a positive
relationship between service quality in hospitals, patient satisfaction and
loyalty (Olusoji, 2009:7).Quality often leads to patient satisfaction.
Satisfied patients are more likely to repeat purchases and remain faithful,
which leads to a positive word-of-mouth
10
and an increase in hospital profitability (Desai, 2011:41). In
order to understand satisfaction in health care, researchers have investigated
different service quality dimensions considered to influence patient
satisfaction (Desai, 2011:40).
They developed the SERVQUAL instrument to evaluate service
quality. The model has been used and adapted to a broader range of service
industries, including in hospital settings. SERVQUAL is used to assess the gap
between patients' perceptions, expectations of services and the actual service
performance. (Yesilada & Direktor, 2010:963).The model is composed of 22
pairs of Likert-scale statements built around five service quality elements
such as tangibility, reliability, responsiveness, assurance and empathy to
evaluate quality in health care (Desai, 2011:42). These service quality
dimensions are reviewed by patients and considered to influence patient
satisfaction (Desai, 2011: 40).
Tangibility: It encompasses the physical evidence of
a service (Holder, 2008:47).This refers to variables ranging from physical
environment, biochemistry laboratories, hospital rooms, cleanliness in
hospitals, to equipment like scanners, X-rays, tread- mills, computers,
appearance and uniforms of medical personnel. Tangibility is crucial in the
delivery of services in hospitals as it can reduce the gap between patients'
expectations and the actual delivery of service (Holder, 2008:23). It provides
a picture of what is inside a hospital and can influence patients' choice when
selecting a health service provider (Zeithaml, Bitner & Gremler,
2006:319).Tangibility is viewed to significantly influence patients'
satisfaction level with services provided (Rohini, 2006:68).
Reliability: It entails providing regular
performance and dependability (Holder, 2008:47). It refers to the ability of
medical staff to honour their promises and provide the promised services to
patients timely and correctly (Rezaei, Rezaei, Alipour & Salehi, 2011:486).
Such services may include casualty, emergency service and prompt treatment for
instance (Rohini, 2006:68). Reliability is perceived to influence patients'
satisfaction level with care, and constitutes one of the major factors by
patients when selecting a medical service provider (Rohini, 2006:68).
Responsiveness: It is an important constituent of
service quality dimensions. It refers to the readiness of the medical personnel
to assist patients and to offer prompt service (Hernandez et al., 2009:1174).
Such services may include patients' admission, discharge, and excellent
reception. Patients' satisfaction often results from hospitals where employees
are kind, helpful and available to provide quick answers to their
11
needs. Responsiveness is perceived to have an effect on
patients' satisfaction level with services, and is highly regarded to influence
their choice with care in hospitals (Rohini, 2006:69).
Assurance: It involves integrity, trustworthiness
and credibility of medical personnel. It refers to the ability of medical
employees to have patients' best concern at heart (Holder, 2008:47). Assurance
leads to providing trust and confidence to the recipient of the service. This
may result from expertise of medical personnel like their qualifications,
trainings, educational level and their ability to effectively provide services
and interact with their patients in hospitals. Assurance is seen to determine
patients' choice with services, and to considerably influence their
satisfaction level with medical care (Rohini, 2006:69).
Empathy: It refers to the ability of medical staff to
provide care, assistance and attention to patients. Physicians should be able
to assist patients during the process of care, and should be able to understand
their needs, listen to and notify them about their health concerns (Markovic
& Raspor, 2010: 197).
As a result, the level of attention and emotional support
experienced by patients in health care can impact on their satisfaction level
with services. This can in turn influence their choice when selecting a
hospital (Rohini, 2006:69).
These five dimensions of quality are known to be linked to
patients' satisfaction and to influence their choice when selecting a medical
facility in general (Desai, 2011: 41). However, there is no clear understanding
of which dimension is mainly influencing patient satisfaction and choice for
the selected hospital in this current study.
1.8 RESEARCH METHODOLOGY
In this part, the methodology for the study and the reasoning
for selecting a research design are verified. It is crucial to differentiate
research design and methodology since the two notions are independent, while
still interconnected. However, the relationship between the two concepts is
often difficult to establish. Holder (2008:5) notes that a research design is a
master plan that indicates how research has to be performed. Research design
and research methodology are two distinct dimensions of research, though many
people often confuse them (Babbie & Mouton, 2009:74).
12
The following research design is set in order to achieve the
objectives of the study as mentioned in section 1.5:
The research is first build around a literature study to
provide a background related to the empirical part of the study. In this
section, a fundamental review of related concepts will be performed. A number
of research propositions will be carried out from the literature findings. This
research was built upon primary and secondary data, and the design is of a
quantitative nature. The element to assess in the study is «individuals
and individuals' behaviour. The research was performed using self-administered
survey questionnaires by respondents for the research. The questionnaires are
based upon the literature study and pretested with a small number of
individuals from the sample with attributes comparable to the respondents of
the research.
«A population for a research refers to a population
group where the study intends to draw conclusions from» (Babbie &
Mouton, 2009:100). The population for the intended research include all
existing patients of the military hospital in Libreville, Gabon,18 years or
older, males and females, who have experienced services at the military
hospital for at least one night. These population elements are chosen mainly
because during a telephone interview conducted on 4 February 2012, an employee
at the military hospital hospital stated that over 80 per cent of patients
attending the military hospital were overnight patients. These patients have
experienced a wider range of services provided such as quality of hospital
rooms, quality of care, quality of medical diagnosis and treatment.
This makes it easy for the researcher to investigate the
choice factors for selecting a military hospital in Libreville, Gabon.
Therefore, all day patients attending the military hospital will be excluded
from the study population. The probability sampling technique was used to
choose respondents in the study. Data gathered from the study will be coded and
recorded into a statistical software package. Findings will be evaluated using
advanced statistical techniques and a number of Tables. The methodology chapter
will provide a further view regarding the method, techniques and instruments
utilised.
In this study, the following statistical methods were chosen
for their suitability to examine the hypotheses in the study. These methods
encompass frequency Tables, measurement of the mean, measures of dispersion
that comprise standard deviation, and descriptive statistics. The research
instrument was verified for its validity and
13
reliability(Refer to Section 4.2.5.7). All evaluations were
performed by the University of Johannesburg's Statistical Consultation Service
(STATKON) and calculations were performed using SPSS.
1.9 ETHICAL CONSIDERATIONS
As required in Brizee (2010), the following ethical
considerations will be observed by the researcher:
? The researcher should obtain permission from the
institution where the study is intended to be done, to conduct his research.
? The researcher should not cause any offence or attempt to
hurt respondents in his study. Therefore, he should carefully select questions,
in order to avoid any offense to his subjects during interviews.
? The researcher should avoid using his own opinions to
influence the interviewees in the study. Therefore, he must remain more
objective than subjective.
? Unless with the permission of the interviewee, the researcher
should keep the identity of respondents to the research anonymous.
1.10 LIMITATIONS OF THE STUDY
The study will only focus on a sample of 200 patients and can
therefore not be seen as representative of all patients attending the military
hospital. The study focuses on identifying the variables influencing patient
satisfaction at the military hospital in Libreville, Gabon. Therefore the study
cannot be seen as representative of services in the entire health care
industry. The use of a survey is also a limitation to the study. The respondent
responses might be bias and they might deliberately falsify their answers.
Future research may include a bigger sample and include other medical
facilities in Gabon.
14
1.11 DIVISION OF THE STUDY
Chapter 1
This chapter provides the introduction and background to the
study. The formulation of the research problem, the objectives and the
hypotheses of the study will be outlined. Similarly, the purpose and
significance of the study, reviewing of the literature, the scope and
limitation of the study were presented in this chapter.
Chapter 2
Chapter two describes the state of health care in Africa and
in Gabon in particular. In addition, it will discuss health care development
strategies in hospitals, and furthermore, focus on how the military hospital
has been operating since the facility was established.
Chapter 3
Literature in this chapter will give insight into the aspects
of services marketing in organisations and in the health care industry, and how
it can benefit organisations through improving services quality that meets
customers' expectations and leads to customer satisfaction. This chapter will
also discuss service quality in organisations as well as in the health care
sector. It will investigate at how quality services can lead to customer
satisfaction and profitability. Aspects such tangibility, reliability,
responsiveness, assurance and empathy will be discussed.
Chapter 4
In this chapter focus shall be placed on the research
methodology and design to be followed to achieve the research objectives. In
other words, emphasis will be on the research method, research format, research
technique, population, and the sampling methodology which includes sample size,
sampling type and sampling technique and data analysis.
Chapter 5
The analysis and interpretation of data will be presented in
the chapter. The research finding and interpretation of data will be presented.
The results obtained will be compared with the findings of the already
published empirical studies and the literature review on which the study is
based.
15
Chapter 6
In this chapter, the researcher will come to conclusions and
make recommendations. From the results it will be possible to determine whether
the research objectives as stated in the first chapter were achieved, and if
the problem statement as described is relevant. Conclusions will be drawn and
meaningful recommendations made.
1.12 TERMINOLOGY
Gabon
The country is located in the central part of the African
continent with official language French, spoken by the majority of the
population. The country shares borders with Equatorial Guinea, the Republic of
Congo and Cameroon. The country has a population of around 1 545 255. Most of
the population is concentrated in Libreville, the biggest city and the main
capital as well (Country Brief Gabon, 2010).
Military hospital
It refers to a medical facility inaugurated in 2005 in
Libreville. The main purpose is to offer better health care services to
patients. The military hospital is equipped with high quality materials and
composed of a range of qualified staff including general practitioners,
specialists and nurses. The facility is characterised by various departments
including the department of surgery, ophthalmology, radiology, cardiology,
endoscopy, angiography and a general medical practice department (Hôpital
d' instructions des armées présentation, 2011).
General hospital
It is also known as the Libreville Hospital Centre. It is
regarded as one the oldest and best known public hospitals in the country. It
was established in Libreville by the government and the main objective of the
facility was to provide health care services to a larger number of the
population at a lower cost compared to private health care systems.
Service quality
16
Service quality is a complex approach because of its
intangible, heterogenic, inseparable and perishable nature (Naik, 2010).
Service quality should be closely associated to the user's perceptions and
expectations of the service provided by an organisation that depends on his or
her prior expectations of the service. In this regard, services that exceed his
expectations will be perceived as outstanding, those that match his
expectations will be perceived as satisfactory and those not meeting his
expectations will be classified as poor (Al Sharif, 2008:2).
Patient satisfaction
Patient satisfaction refers to a positive attitude towards
services provided by a medical facility. Patient satisfaction can be perceived
both at a cognitive and emotional angle and linked to prior experiences,
expectations and referral from other individuals. It is used to assess the
level of service in medical settings, as well as to compare medical programmes.
Patient satisfaction evaluation helps to identify which area of service quality
needs improvement (Al Sharif, 2008:21).
Tangibility
It encompasses the physical evidence of a service (Holder,
2008:47).This refers to variables ranging from physical environment,
biochemistry laboratories, hospital rooms, cleanliness in hospitals, to
equipment like scanners, X-rays, treadmills, computers, appearance and uniforms
of medical personnel. Tangibility is crucial in the delivery of services in
hospitals, as it can reduce the gap between patients' expectations and the
actual delivery of service (Holder, 2008: 23). It provides a picture of what is
inside a hospital and can influence patients' choice when selecting a health
service provider (Zeithaml, Bitner & Gremler, 2006:319). Tangibility is
viewed to significantly influence patients' satisfaction level with services
provided (Rohini, 2006:68).
Reliability
It entails providing regular performance and dependability
(Holder, 2008:47). It refers to the ability of medical staff to honour their
promises and provide the promised services to patients timely and correctly
(Rezaei et al., 2011:486). Such services may include casualty, emergency
service and prompt treatment for instance (Rohini, 2006:68). Reliability is
perceived to influence patients' satisfaction level with care, and constitutes
one of the major factors by patients when selecting a medical service provider
(Rohini, 2006:68).
17
Responsiveness
It is an important constituent of service quality dimensions.
It refers to the readiness of the medical personnel to assist patients and to
offer prompt service. Such services may include patients' admission, discharge,
and excellent reception. Patients' satisfaction often results from hospitals
where employees are kind, helpful and available to provide quick answers to
their needs. Responsiveness is perceived to have an effect on patients'
satisfaction level with services and is highly regarded to influence their
choice with care in hospitals (Rohini, 2006:69).
Assurance
It involves integrity, trustworthiness and credibility of
medical personnel. It refers to the ability of medical employees to have
patients' best concern at heart (Holder, 2008:47). Assurance leads to providing
trust and confidence to the recipient of service. This may result from
expertise of medical personnel like their qualifications, trainings,
educational levels and their ability to effectively provide services and
interact with their patients in hospitals. Assurance is seen to determine
patients' choice with services, and to considerably influence their
satisfaction level with medical care (Rohini, 2006:69).
Empathy
It refers to the ability of medical staff to provide care,
assistance and attention to patients. Physicians should be able to assist
patients during the process of care, and should be able to understand their
needs, listen to and notify them about their health concerns. As a result, the
level of attention and emotional support experienced by patients in health care
can impact on their satisfaction level with services. This can in turn
influence their choice when selecting a hospital (Rohini, 2006:69).
1.13 CONCLUSION
This chapter provided an outline of the study by discussing
the background of the research, problem statement, research objectives,
hypotheses and a literature review. In addition, a brief discussion of the
research methodology and design was included in the chapter. Lastly, ethical
considerations, limitations of the study, the division of the research and
terminology were presented as well.
18
Chapter Two concentrates on the research context of the study.
It will provide a detailed description of the state of the health industry in
Africa and in Gabon in particular. In addition, it will discuss health care
development strategies in hospitals, and furthermore, focus on how the military
hospital has been operating since the facility was established. A summary will
be provided at the end of the chapter.
19
CHAPTER TWO: THE HEALTH CARE INDUSTRY IN AFRICA
AND
GABON
2.1 INTRODUCTION
Investigating health industry in Africa and particularly in
Gabon is vital to understand the state of health and to promote policies to
enhance health services on the entire continent. Superior health services can
lead to a higher level of patient satisfaction and retention. This is
particularly important since patients satisfied with services are more likely
to repeat purchases, to remain loyal and to follow the medical recommendations
(Olusoji, 2009:16-17). Exploring health services at the military hospital in
Libreville, in Gabon is crucial to determine strategies that could be
recommended to the other hospitals in Gabon, as well as hospitals in other
African countries to improve their service quality and enhance their patient
satisfaction. This chapter explores and analyses the nature of the healthcare
system in Africa with a specific focus on the military hospital in Libreville,
in Gabon. This research may help hospital executives to determine problems
related to poor health services delivery and to address these issues more
efficiently.
This chapter consists of six main sections. These are an
introduction to the health industry in Gabon and Africa, the relevance of the
state of health in Africa to detect issues related to poor health services
performance in the continent. Subsequent to this discussion, the chapter also
focuses on the health development initiatives in central Africa, the health
indicators in Gabon, the organisation of the military hospital in Libreville,
Gabon, followed by a conclusion.
2.2 HEALTH CARE STATUS IN AFRICA
African countries such as Cameroon, Democratic Republic of
Congo, and Equatorial Guinea have a critical and pathetic health care system
that requires attention. Health data for the continent indicates that Africa
loses about one out of six children before they reach five, who die from
sicknesses that could have been avoided by vaccines. In addition, one pregnant
woman dies each two minutes from poor pregnancy and delivery
20
care in hospitals. This raises concerns about the state of
health system in the continent (Health, 2007:19).
Another concern is health care associated infection also
known as (HAI), which is one of the major concerns within most African
hospitals. HAI is described as an infection arising in a patient during the
process of care in a medical institution. Such infection was not diagnosed
during the time the patient was admitted in the hospital. This encompasses
infections acquired while patients were receiving care. These infections may
often manifest after days or even weeks after discharge. Medical employees may
usually be affected by these infections as well, caused by multi resistant
pathogens. Patients' prolonged hospital stay is often regarded as a risk factor
of contracting health care associated infections. This usually results in
excessive costs and may sometimes cause patient's death. HAI is a major issue
in most African states such as in Republic Democratic of Congo and Gabon, where
it affects five to 15 per cent of people admitted in standard wards and as many
as 50 per cent of people admitted in intensive care unit (Nejad et al.,
2011:757). In developed states such as Germany and the United States, control
systems like the German hospital infection surveillance system or the National
Healthcare Safety Network of the United States of America, exist to supply
reports on the prevalence of health care associated infections on a regular
basis. However, in most African countries, such initiative is often taken too
lightly or even neglected. Diagnosing HAI remains a difficult task since it
involves adequate know-how and resources. In addition, medical staff shortage
in most hospitals leads to poor infection control practices, and a lack of
related policies, awareness and skilled professionals also increase the
magnitude of the problem (Prescott & Kruk, 2012:646).
African states have raised concerns to cooperate in order to
restructure the state of their healthcare systems. The New Partnership for
African Development (NEPAD) is developed to consolidate health organisations in
the continent. It encourages collaboration and communication among health
service providers and local societies. Its goal is to alleviate spread of the
HIV/Aids pandemic and other challenges affecting the continent (Health,
2007:19).
Most African countries have taken positive steps to improve
national health strategies as recommended by the World Health Organisation
(WHO). However, only a few of them have recently taken initiatives to revise
their healthcare policies, such nations include Burundi, the Central African
Republic, Mauritania, Tanzania and Gabon (Health, 2007:19).
21
2.3 HEALTH DEVELOPMENT INITIATIVES IN CENTRAL AFRICA
A few organisational health institutions have erected in
Central Africa to promote partnership, training, economic and health
development in member countries of the organisation.
? The OCEAC
The OCEAC (Organisation for the fight against endemic
diseases in central Africa) was established in 1963 in Yaoundé, the
headquarter of the institution. The organisation regroups six central African
states such as Gabon, Congo, Central African Republic, Cameroun, Chad and
Equatorial Guinea which lately joined the group. The organisation's major
priorities are to organise public health strategies and programmes, to take
part in education and training program of medical employees as well as to
organise research projects carried out by national institutions in member
states. In addition, the organisation seeks to share medical knowledge and
skills among health service providers in the region and to enhance public
health awareness so to improve emergency health responses in member countries
of the organisation. The OCEAC is currently involved in several health projects
in the central African region such as: The Sub-Regional Program for HIV and
AIDS and the Harmonisation Program for Pharmaceutical Policy (Organe
exécutif de la CEMAC, 2012).
? CEMAC
The CEMAC (Central African Economic and Monetary Community)
was established in 1983. It aims to support economic growth, cooperation and to
improve living conditions of people in member countries. The organisational
main objectives are to create a Central African Common Market and to enhance
public health systems in the region. In 2009, CEMAC made a contribution of 23
million Euros with the aid of Germany to fight HIV/Aids spread in Central
Africa (Bourgarel, 2010:11).
? The CAMES
The CAMES (Conseil Africain et Malgache pour l' Enseignement
Supérieur) is perceived as an intergovernmental institution composed of
17 African states. It was established in 1968 to regulate the manner in which
health institutions as well as
22
universities in emerging African states were run. The
organisation's objectives are to sustain partnership and communication, to
promote a scientific and cultural collaboration, as well as to ensure
dissemination of all academic and research publications between member
countries. Additionally, health employees and researchers in member states are
consistently examined by CAMES before they can be promoted in their workplace
(CAMES, 2012).
? The CIESPAC
The CIESPAC (Centre Inter- Etats d'Enseignement
Supérieur en Santé Publique d' Afrique Centrale) is based in
Yaoundé, Cameroon. Its objective is to provide public health teaching to
medical employees and executives in member countries. The organisation offers
various programmes such as the professional diploma in public health primarily
targeted at hospital executives. The course offers advanced management skills
to medical managers to transform health systems in the region.An audit
regarding the success of these three organisations was presented during the
seventh Summit of the Central African region in 2008, in Equatorial Guinea. The
results indicated that there was an increase of the availability of medical
facilities in the region; the number of hospitals expanded from 6 per cent in
1990 to 11 per cent in 2008 (Bourgarel, 2010:11).
Furthermore, these organisations also enabled scientific and
medical research between some regional countries. This resulted in the creation
of the Elf Rafa Medical Centre in 2006 in Libreville, in Gabon. The facility
was established with the alliance between Gabon and its direct geographic
neighbour Cameroon to undertake research in order to tackle the spread of
malaria in the region (Programme Economique Régional de la CEMAC,
2009:12). However, despite these improvements, there are still concerns about
the quality of medical services in most central African countries. This is
because there have been little research on patient satisfaction within medical
organisations to pinpoint problems related to poor service performance (Health,
2007:20).
Given these facts, the present research would be necessary to
identify and address issues related to poor service quality.
23
2.4 HEALTH SERVICE QUALITY IN GABON
The health system in Gabon includes: the traditional health
sector, and the two major types of service providers namely the civilian public
sector which is part of the public health and hygiene ministry, and the private
health sector (Bourgarel, 2010:9).In the traditional health sector, health
services are often provided by private individuals usually known as
`marabouts'. Traditional health services make use of traditional plants and are
practised in most villages within the country (Global Health, 2012).
In the public health sector, health services are usually
offered by the state or government. Medical personnel in public hospitals are
often employed by the government. The state is the main provider of resources
and finances in public hospitals; it ensures control over the delivery of
medical care to the people. In the private health sector, medical services are
delivered by private entities, different from the government. Private agents
have control over resource allocations and finances in private hospitals.
Employees in private health care are often employed and remunerated by private
units (National Department of Health, 2006).Despite massive transformations in
the medical industry to force executives of both private and public hospitals
to improve service quality in hospitals, there is still a huge gap between
quality service delivered by private and public institutions (Holder, 2008:59).
Given the fact that competition has increased in the Gabonese health sector and
that health service quality has become crucial to increase market share, this
study will focus on health services. It is worth investigating medical services
since it may help to develop strategies to enhance health services in hospitals
(National Department of Health, 2006).
2.4.1 Public health development initiatives in
Gabon
Public health is dominating in Gabon, however, accessibility
and availability of proper medical services are mainly found in urban districts
compared to rural regions. Hospitals in urban districts are more organised with
more resources and technical know-how (Bourgarel, 2010:10). Over 60 per cent of
public hospitals and clinics are located in major cities such as Libreville,
Port-Gentil and Franceville. These facilities also receive more equipment, as
well as human and financial resources from the state. However, small health
facilities like Mother and Child Centres, Primary Care Health and Health
Medical Centres are usually found in rural regions. They are usually
characterised by
24
lack of drugs and medical equipment availability. In fact over
70 per cent of medical personnel such as physicians, nurses, midwives and
pharmacists are located in urban districts' hospitals (National Department of
Health, 2006).
To fight the spread of HIV/Aids, tuberculosis, malaria and
sexually transmitted diseases (STDs), the government created 17 national health
control programmes in both urban and rural districts between 2009 and 2010. The
goal is to assess the spread of these infections and to establish an effective
vaccination programme of the population. In addition to these efforts made by
the government, the Public Health and Hygiene Ministry established the CENAREST
(National Centre for Scientific and Technologic Research) programme to promote
medical and research training in the industry (Bourgarel, 2010:10).
The CIRMF (International Medical Research Centre of
Franceville) is another initiative established in 1979.The programme was made
possible by various international agents such as the World Health Organisation
(WHO), the Centre de Coopération Internationale en Research Agronomique
(CIRAD), the Institut de Recherche pour le Development (IRD), the Pasteur
Institute, the American Centre for Disease Control and Prevention (US CDC) and
various European, American and Asian universities. The programme aims to
investigate factors causing infertility in people in the Central African
region. Additionally, CIRMF expanded its research to investigate regional
infections like HIV/Aids, trypanosomiasis, malaria and the fatal Ebola and
Marburg viruses that severely affected the country lately (Leroy &
Gonzalez, 2012:159). The international non-governmental agencies have also
taken part in research for diseases in the country. Such organisations include
the Wildlife Conservation Society (WCS) and the Zoological Society of London
which are investigating co-operatively on diseases affecting great apes
(Bourgarel, 2010:10).
2.4.2 Private sector development initiatives in
Gabon
Since 2010, various efforts have been made to support private
investment initiatives by increasing the number and the size of private
organisations. The country is aware that export of oil, its main natural
resource, will not be the source for economic expansion eternally. Recent
strategies have been made to encourage the development of the private health
sector. Private hospitals have been lacking and almost inaccessible over
25
the years. The reason was that these facilities often lacked
proper strategies. As a result, more policies to build collaboration and to
attract investors were developed. The aim was to provide more private,
ultramodern hospitals to the population (Health, 2007:22). As a result, the
country has built relationship agreements with emerging countries like China,
India, Morocco and Singapore to boost investment in the private sector
including private hospitals and to create more jobs (Gabon, 2011:11).
Despite efforts made since 2009 by the Agence de promotion
des investissements privés (APIP) to support private investment, the
business prospect in the country has been very slow. This has been caused by
corruption, poor governance and the increase in the informal sector (Gabon,
2011:11). Health services in Gabon provide geographic coverage to most regions
of the state. The aim is to give people better access to health information and
efficient controlling of emerging sicknesses. Though the population of Gabon is
dispersed equally between cities and rural areas, accessibility to health
services is better in cities compared to rural areas, as more resources and
medical infrastructures are located. Though healthcare infrastructures in rural
areas are lacking, the state is trying its best to enhance and supply adequate
health services to the population residing in these rural areas (Republic of
Gabon, 2008: 42).
In Gabon, patients are usually required to pay for the
services delivered by medical professionals. Drugs are often costly in the
country and are usually not available in rural areas. Medical facilities in
rural areas are often badly equipped; patients usually need to go to the
closest city to get their medication. Instead of going to a city doctor, some
people may rather choose alternative treatment, like going to a local
traditional healer instead. In the case of severe medical conditions, people
can only be given care in Libreville, the capital city, where proper hospitals,
clinics and equipment are accessible. Public hospitals in Gabon are usually not
up to international standards, compared to a few private hospitals such as El
Rapha or the military hospital in Libreville. As a result, public health
facilities generally provide poor medical services to patients in contrast to
private ones. There are currently 49 available doctors per 100 000 people in
the country; this makes Gabon to be positioned number 9 out of 52 African
states in terms of doctor to patient ratio (Global Health, 2012). Private
clinics and hospitals are accessible in bigger cities, and they offer a broader
range of superior health services. However, these facilities are costly to the
population and hospitals generally require immediate cash payment before
patients can be treated and/or admitted. People either pay cash for treatment
or use a medical cover plan to have access to medical services.
26
However, two out of three of the people in Gabon live below
the poverty line, as a result, only a few people can actually afford access to
private health care services (Gabon Poverty and Reduction Strategy Paper,
2012:21).
Malaria is regarded as the major pandemic that affects most
people living in the country. HIV/Aids is also perceived as a continuous threat
in Gabon. There are frequent occurrences of Ebola virus that strike people
living in rural areas. This is usually caused by individuals who maintain close
interactions with infected animals. Having a medical insurance plan in Gabon is
regarded as one of the best options to tackle accidents, sicknesses and
emerging pandemics that can affect the population at any given time. Medical
cover policies generally provide customised individual needs to suit
individuals, families and groups. In addition, they can provide benefits for
inpatient, outpatient, dental, maternity, travel and many more conditions
(Global Health: 2012).
Health indicators data reports 500 nurses, 30 general
practitioners, 20 laboratory employees, 5 dentists, 5 pharmacists and 10
medical specialists for every 100 000 people. HIV/Aids occurrence rate in adult
population (15-49 year-old) is 5.9% which is 0.9% above the average sub-Saharan
region. Among the 49 000 of the population living with AIDS, 27000 (15 years
and older) are females and 2 300 (0-14years) are children. About 18 000
children in Gabon have lost one or both parents due to HIV/Aids. The occurrence
of tuberculosis is 410 per 100 000 individuals, and 41 out of 100 000 of them
die of the disease. The occurrence of diabetes among the adult population (20
years and older) is 4.4% which is 1.2% above the average rate on the continent.
158 out of 100 000 people die of cancer and 410 out of 100 000 people have died
from heart-related sicknesses (Gabon, 2010:13).
The International Diabetes Federation (2010) reports that
over 33 000 people suffered from diabetes and over 600 died from complications
caused by the disease in 2010. The occurrence of obesity was 2.3% for men and
15.5% for women. Over 380 000 people contracted malaria and 1 255 individuals
died of the disease during the same period. In terms of maternity death rate,
the country is still far behind other African countries such as Mauritius for
instance. Maternal death rate ratio in Gabon was 470 per 100 000 women giving
birth in 2011, in contrast to 24 per 100 000 women in Mauritius. This raises
awareness of the World Health Organisation which indicated that the maternal
mortality rate in Gabon could decrease by ensuring that pregnant women
27
and children could have access to adequate health care
services. This suggested that providing each woman with skilled care through
pregnancy and emergency, this assistance could significantly reduce the rate of
women and children mortality in the country (Gabon Poverty and Reduction
Strategy Paper, 2012:20).
2.5 IMPLICATIONS OF HEALTH SERVICE QUALITY IN GABON
Service quality in hospitals is described as a service which
has the ability to satisfy a patient's needs. Patients' perception of medical
services plays a vital role in his or her choice for the medical service
provider (Vanniarajan & Arun, 2010:1). The raise of public awareness about
service quality has also increased concerns for health service quality in
Gabon. As a result, most people are currently seeking hospitals that provide
superior care. Since 2003, patients' expectations of quality care have
increased at a faster rate. Service quality in hospitals has become part of the
governments' main agenda, and it has been enforced by the World Health
Organisation. As a result, the government has to ensure that service quality
within hospitals in Gabon comply with international standards. This is regarded
as a pre-requisite for the local government to be provided with financial
assistance by international aid organisations for the building of more
hospitals in Gabon. During a telephone interview conducted on 3rd
April 2012, a medical personnel at the military hospital stated that improving
service quality in hospitals in Gabon has become vital to enhance the
credibility of the country's health care system to the world. This in turn may
attract more patients locally and internationally.
2.6 HEALTH DEVELOPMENT INITIATIVES IN GABON
Government expenditure on health per capita amounts to $130
per person, which represents 4.5 per cent of the national Gross Domestic
Product. This ranks the country third after Seychelles ($382) and Botswana
($135) per person. Unfortunately, this investment has often not been utilised
adequately to its full potential. Financial resources have to be properly
managed in order to meet the country's health development initiatives. Medical
services in the country lack innovations and they can no longer address the
needs of the people (Health, 2007:21).
28
A transformation in the health care industry is required to
achieve the four major target initiatives such as raising the number of both
private and public hospitals so that the entire population can have access to
quality care. This includes enhancing the health of mothers, newborns and
children, since healthy mothers are more likely to have healthy babies and
healthy children are the future of the country. Access and affordable medicines
need to be provided to all people and a universal medical cover based on the
European model has to be implemented to the whole Gabonese population. The idea
is to increase the number of people's accessibility to proper medical services
(Health, 2007:21).
The government of Gabon in collaboration with the French Aid
Agency, the African Development Bank and the United Nations Population Funds
has sponsored in total 14 hospitals to enhance mothers, newborns and children's
health in the country. This initiative is aimed at recruiting more medical
experts such as gynaecologists and obstetricians to improve women's health. In
addition to this, the local government planned to create more health care
infrastructures that include 9 of the local hospitals, 46 health centres and a
network of 455 rural health clinics spread around the country by the end of
2020. Since 2007, women and children`s health has become one of the major
priorities in the country's health system. Enhancing maternal and children's
health is a Millennium Development Goal. As a result, that strategy has become
a priority in the country since 2007 (World Health Organisation, 2007:22).
Vaccination campaigns against poliomyelitis in infants and
tuberculosis were other initiatives undertaken by UNICEF to improve people's
living conditions in Gabon. A common problem affecting the adult population was
the spread of malaria and gastrointestinal diseases in the country since 2005.
In the northern province of Gabon in Woleu-Ntem, over 60 per cent of the
patients admitted in hospitals suffered from infections caused by mosquitos.
Fever and acute diarrhoea were among other major sicknesses affecting adults
and the young population as well. Libreville, the main capital became mostly
affected with 8.1 per cent of people affected by fever and diarrhoea. To tackle
the spread of the pandemic, a mobile medicine strategy was developed by the
government to prevent further spread of these sicknesses. This suggested that
more medical professionals would travel around the country to deliver care to
outpatients and undertake vaccination drives. These mobile doctors were
employed to provide health services coverage in the entire country, including
the less populated regions. The major
29
sicknesses targeted represented poliomyelitis, tuberculosis,
diarrhoea, HIV/aids disease and malaria (Health, 2007:21).
An additional strategy was developed by the government to
build a university teaching hospital near the main capital of Libreville in
2007. This was done in collaboration with the Japanese medical group,
Tokushakai that has a particular interest in building hospitals in developing
countries. Cooperation agreements have also been established with countries
such as France, Canada and Egypt to provide adequate training and expertise to
home-grown medical professionals. This resulted in an increase of 34 per cent
of the human resource for the medical sector from 1999 to 2007. Since 2003, a
particular attention was given to the training, education, remuneration and a
continuing deployment of the medical professionals in the Gabonese Health Care
System. In 2007, over 200 medical professionals were recruited from Egypt and
Cuba to tackle the personnel shortage in the health care sector (World Health
Organisation, 2007:23).
In 2011, the government developed an important strategy to
tackle the high cost of medicines in the country. The Turnkey laboratory was
established near the main capital of Libreville to tackle malaria and HIV. The
project aimed at producing generic pills to the population. Government
expenditures to establish the laboratory amounted to approximately 6.5 million
euros. Building this facility was part of the country's health care strategy to
enable patients at all economic levels to access adequate treatment. The
initiative suggested that the newly established laboratory aimed to fill the
demands of the people of Gabon, but it could also fill demands of the whole
central African region. With a total production of 200 000 drugs every hour,
the laboratory may actually be able to supply drugs to all the African states
that are part of Central African Economic and Monetary Community (CEMAC) with a
global market of 30 million people (Gabon Poverty and Reduction Strategy Paper,
2012:23). The new laboratory provides paracetamol, tuberculosis and
anti-malaria drugs which actually encounter no resistance. The initiative was
seen as an innovation in the pharmaceuticals industry in the central African
region. The facility includes over 30 Gabonese health professionals, and raw
materials quality control is conducted at a chemical plant in France (Health,
2007:23).
30
2.7 THE MILITARY HOSPITAL IN GABON
The idea to establish the military hospital dated back from
the late 1970s to early 1980s.The project was inaugurated in 2005, and the
facility has been officially operating since 31 December 2007.The initial
ideology was to provide medical services merely to the military forces in the
country. This idea was later transformed in a way anyone can have access to
medical services provided by the medical facility. The military hospital was
financed by major international organisations such as the French Collaboration
(F.C), regarded as one of the main contributors. The hospital team is a mixture
of local and international qualified medical professionals, mostly French
nationals. Each department within the hospital is equipped with advanced
medical equipment ranging from ultramodern air conditioners, computers, X-ray
machines, scanners, audiometric, echo graph, electrocardiograph, radiology,
endoscope to echocardiograph machines (Historique, 2010).In addition, five
ambulance vehicles and a helicopter are available 24 hours a day and seven days
a week to deal with emergencies (Service d'accueil, 2010).
The hospital executive panel is composed of the Chief Medical
Director (CMD), who is both a medical specialist and the general director of
the hospital, the head of the department of radiology, the head of department
of internal medicine and the head of the department of Ear, Nose and Throat as
well as medical specialists. There are eight main clinical departments in the
military hospital. Each of these departments will be briefly highlighted in the
following Tables (Historique, 2010).
Table 2.1: Department of emergency
DEPARTMENT OF EMERGENCY
It works 24 hours a day and seven days a week. An ambulance
vehicle and a helicopter are available to patients in case of emergencies. The
department delivers a fast and reliable service to patients (Service d'accueil,
2010).The department of emergency is composed of:
A reception
This provides excellent services to patients.
31
A consultation and emergency room
This facility is able to deal with all types of emergencies
ranging from
medical to chirurgical emergencies. It is equipped with
modern
technologies such as electrocardiographs and echocardiographs
to
provide assistance to patients in critical conditions (Service d'accueil,
2010).
|
A temporary admission room
Patients can first access the temporary admission room while
they wait to be transferred to the emergency room. The room has a total
capacity of 10 patients and is divided into two sections to separate male and
female patients. The facility is able to provide intensive care services
(Service d'accueil, 2010).
|
A room to disinfect patients
In that room patients are cleared from any bacterial
transmitted infection before they are moved to the temporary or emergency room
(Service d'accueil, 2010).
|
A surgery room
Patients admitted in that facility require an operation
(Service d'accueil, 2010). The emergency team is composed of medical experts
that shift day and night. This includes general practitioners, specialists,
anaesthetists, paramedics and nurses (Service d'accueil, 2010).
|
|
Table 2.2: Department of medical analysis
DEPARTMENT OF MEDICAL ANALYSIS
The department of medical analysis includes subunits such as
haematology, immunology, bacteriology and mycology.
Haematology
This unit includes up-to-date medical equipments to analyse
blood composition and to detect any anomalies or sicknesses in blood
|
|
32
(Laboratoire d'analyses médicales, 2010).
|
Immunology
This unit aims at detecting and analysing viral, parasitic
and bacterial infections found in blood. The unit addresses three major forms
of health issues such as: viral serology (which includes HIV/Aids and hepatitis
B and C), parasitic serology (which includes bilharzia and toxoplasmosis) and
bacterial serology (that comprises syphilis and chlamydia). In addition, this
unit works jointly with the HIV/Aids national programme in the fight against
AIDS (Laboratoire d' analyses médicales, 2010).
|
Bacteriology
This section analyses viral and parasitic infections in
urine. Additionally, women can also be treated for early signs of breast and
womb cancer (Laboratoire d'analyses médicales, 2010).
|
Mycology
This unit includes medical equipment such as advanced
microscopes to detect viral and parasitic infections in blood. As a result,
patients are often successfully treated and cured from trypanosomes,
cryptosporidiosis and other related bacterial infections (Laboratoire
d'analyses médicales, 2010).
|
|
Table 2.3: A pharmacy
A PHARMACY
A pharmacy is located within the military hospital, and
medicines are available to patients after they have been consulted. A range of
tablets is available to treat most diseases, and medicine stocks are frequently
renewed (Pharmacie hospitalière, 2010).
33
Table 2.4: Department of internal medicine
DEPARTMENT OF INTERNAL MEDICINE
|
It includes a head of department, and a team of medical
specialists such as
dermatologists, cardiologists and nurses. The department of
internal
medicine also has a programme to provide teachings and trainees to
medical students (Médécine interne, 2010). The department
includes four main units:
|
A unit that treats patients suffering from the most common
diseases affecting the country such as malaria and yellow fever. The facility
has a capacity of 200 people (Médécine interne, 2010).
|
A unit that treats only patients suffering from heart-related
diseases. A team of cardiologists is constantly available to provide intensive
care to admitted patients. The unit has a total capacity of 70 people (Medicine
interne, 2010).
|
A unit that monitors the health of patients who are admitted.
The unit comprises of echocardiograph and electrocardiograph equipment to
assess patients' health (Médécine interne, 2010).
|
A VIP unit which is only designed for special clients such as
heads of states, ministers and other important clients.
|
|
Table 2.5: Department of surgery and
orthopaedic
DEPARTMENT OF SURGERY AND ORTHOPAEDIC
Patients who require surgery are often admitted in that
facility. The department is known to provide surgery of the digestive system as
well as urologic, visceral and thoracic surgery. The facility has a maximum
capacity of 32 patients (Chirurgie générale,
2010).
34
Table 2.6: Department of ophthalmology
DEPARTMENT OF OPHTALMOLOGY
|
It includes 3 main units such as:
A consultation room which offers eye tests and treatments to
patients. The unit includes advanced eye equipment and is known to provide
superior services to customers (Ophtalmologie, 2010).
|
A surgery unit where major eye problems such as cataracts and
glaucoms can be removed via surgery (Ophtalmologie, 2010).
|
An admission room where patients in critical conditions can
be admitted. A team of ophthalmologists is available to provide excellent
services to patients. The unit has a maximum capacity of 16 patients
(Ophtalmologie, 2010).
|
|
Table 2.7: Department of Ear Nose and Throat
(ENT)
DEPARTMENT OF EAR NOSE AND THROAT (ENT)
This department is divided into two major units: A unit that
tracks hearing disorders in patients. The facility includes advanced medical
equipment such as audiometers to detect hearing problems in both young and
adult patients (Orl & Ccf, 2010).
A unit that treats throat diseases and speech disorders. That
section encompasses spectrograph equipment to detect and examine anomalies in
the throat and speech of patients. The medical team in that unit comprises
general practitioners, paramedics, nurses and specialists who provide daily
care and assistance to patients. A surgery room is also available to patients
who require a throat operation (Orl & Ccf, 2010).
35
Table 2.8: Department of radiology
DEPARTMENT OF RADIOLOGY
The radiology department includes: a unit for chest
radiology, a unit for bones radiology and an ultrasound room. The facility
includes advanced X-ray and scanner equipment and provides superior services to
patients (Radiologie et imagérie médicale, 2010).
For the purpose of this study, the focus will be on the
Department of internal medicine since during a telephone interview conducted on
4 June 2012 it was regarded as the one receiving the largest number of
patients. Patients in that department were also required to stay over in the
hospital for at least one night.
Table 2.9: Military hospital
DEPARTMENT OF EMERGENCY
|
It is operational 24 hours a day and seven days a week. An
ambulance vehicle and a helicopter are available to patients in case of
emergencies. The department delivers fast and a reliable service to patients.
The department of emergency is composed of a reception, a consultation and
emergency room, a temporary admission room, a room to disinfect patients and a
surgery room (Service d'accueil, 2010).
|
DEPARTMENT OF MEDICAL ANALYSIS
The department of medical analysis includes subunits such as
haematology, immunology, bacteriology and mycology (Laboratoire d'analyse
médicales, 2010).
|
A PHARMACY
A pharmacy is located within the military hospital, and
medicines are available to patients after they have been consulted. A range of
tablets is available to treat most diseases, and medicines stocks are
frequently renewed (Pharmacie hospitalière, 2010).
|
DEPARTMENT OF INTERNAL MEDICINE
It includes a head of department, and a team of medical
specialists such as dermatologists, cardiologists and nurses. The department of
internal medicine also has a programme to provide teachings and training to
medical students. The
department includes four main units: A unit that treats patients
suffering from the
|
|
36
most common diseases affecting the country such as malaria
and yellow fever; a unit that treats only patients suffering from heart-related
diseases, a unit that monitors the health of patients who are admitted, and a
VIP unit which is only designed for special clients such as heads of states,
ministers and other important clients (Médécine interne,
2010).
|
DEPARTMENT OF SURGERY AND ORTHOPAEDIC
Patients who require surgery are often admitted in that
facility. The department is known to provide surgery of the digestive system as
well as urologic, visceral, and thoracic surgery. The facility has a maximum
capacity of 32 patients (Chirurgie générale,
2010).
|
DEPARTMENT OF OPHTALMOLOGY
It includes 3 main units such as: A consultation room which
offers eye tests and treatments to patients a surgery unit where major eye
problems such as cataracts and glaucoms can be removed via surgery, and an
admission room where patients in critical conditions can be admitted
(Ophtalmologie, 2010).
|
DEPARTMENT OF EAR NOSE AND THROAT (ENT)
This department is divided into two major units: A unit that
tracks hearing disorders in patients and a unit that treats throat diseases and
speech disorders (Orl & Ccf, 2010).
|
DEPARTMENT OF RADIOLOGY
The radiology department includes a unit for chest radiology,
a unit for bones radiology and an ultrasound room (Radiologie et
imagérie médicale, 2010).
|
|
2.6 CONCLUSION
In this chapter, the focus was to investigate the state of
the health industry in Africa and more specifically, in Gabon. The health
development initiatives in central Africa were introduced and the relevance of
organisational health institutions such as OCEAC, CEMAC, CAMES and the CIESPAC
in central Africa was also discussed in details. The chapter discussed the
health indicators in Gabon as well as the quality of medical services delivered
in the country. This enabled the researcher to assess the strengths and
weaknesses of the Gabonese health care system. Following that discussion, a
review of the two major health sectors in Gabon, as well as the health
developmental
37
strategies in the public and private sector were also debated
in order to improve the quality of health in Gabon. The last part of the
chapter provided a discussion of the military hospital in Libreville, in Gabon
as well as a conclusion.
The following chapter will put services marketing, service
quality and customer satisfaction in perspective and the advantages of
implementing these elements to both the customer and the organisation will be
discussed. Chapter Three will also discuss the link between expectations,
customer satisfaction and service quality.
38
CHAPTER THREE: SERVICES MARKETING, SERVICE QUALITY AND
CUSTOMER SATISFACTION
3.1 INTRODUCTION
The purpose of Chapter Two was to examine and have a deep
understanding of the nature of the health system in Africa and more
specifically, in Gabon. It provided an 2overview of health
development initiatives in Africa and concluded with a focus on the military
hospital in Libreville in Gabon. Chapter Three provides a theoretical
discussion of services marketing, service quality and customer satisfaction. It
provides a discussion on the definitions, generic elements and importance of
services marketing, service quality and customer satisfaction. Additionally, a
discussion on the relationship between expectations, customer satisfaction and
service quality will be included in the chapter.
In most countries, people have spent more on services than on
tangible goods. Service companies have become major contributors in the world
economies. They account for more global outputs and provide work for more
individuals than any other sector. By the mid 2000s services represented 33% of
the world's Gross Domestic Product which is about $ 6 trillions of additional
income, down from about 50% in the 1990s. Worldwide services growth is about 3%
more than agriculture which is 1.4%, and the manufacturing industry that is
2.3%. As a result, the services sector expanded significantly from 57% in the
1990s to over 68% in the mid 2000s (World Bank Development Indicators, 2012:1).
Compared to other sectors in the world, the services sector has become the
largest and the fastest growing one. Some of the reasons for such a rapid
growth are mainly due to the increase in urbanisation, privatisation and the
increase in demand for intermediate and final consumer services. Accessibility
of quality services is fundamental for the well-being of people and the
economy. Studies revealed that in most advanced economies, the expansion of the
primary sector which makes use of natural resources such as agriculture,
mining, forestry, oil and gas and the secondary sector that produce
manufactured goods such as goods to the automobile industry, was mainly
correlated to the growth of services such as bank, trade, commerce,
entertainment and insurance services. In most European economies and
39
the USA, the service sector has accounted for more than
two-thirds of these countries' Growth Domestic Product (GDP) (Service Sector
Around the World, 2012).
In Africa, despite many challenges such as poverty,
sicknesses, high mortality rate among children and HIV/Aids affecting countries
like Ethiopia, Somalia and Soudan, the continent's Gross Domestic Product (GDP)
rose significantly from the early 2000's to 2011 which amounted to $1.6
trillion. Since the 2000s, real GDP has increased by almost 5% yearly. This
represents almost more than twice its pace between the 1980s and 1990s.
Africa's growth is mainly due to the primary sector through commodities like
oil and minerals. This represented almost 40% of the global GDP. The remaining
60% contribution to the African GDP comes from secondary sources namely
industry 32% and services 28%. Since the 2000s, the service sector has grown at
a slower pace compared to other sectors in Africa (Leke, Lund, Roxburgh &
Van Wamelen, 2010).
The primary sector is perceived as the main source of
economic expansion in Gabon, with the export of raw material such as manganese,
and timber oil, representing over 43% of the gross domestic product in 2012.
The secondary sector such as manufacturing represented 25%, and services such
as hotels, transport, information, finance and business services represented
over 32% of the country's Gross Domestic Product (Trading Economics, 2012).The
country' s real GDP growth has decreased considerably from 8.6% in 2007 to 4.4%
in 2012. As a result, since 2009, the state has launched various strategies to
improve the country's economy, including boosting the services sector to create
more jobs. These measures led to more employments in some services such as the
hotel and transport industries. This led to a sharp rise of 7% growth in
services over the secondary sector (Gabon Economic Outlook, 2012).
An important approach to assess the structure of a country's
economy is to evaluate the share of its three major sectors namely:
agriculture, manufacturing and services, to see which sector has the largest
total output and employment. Initially, agriculture was perceived as a
country's most important developing sector. But with the increase of the per
capita income, it weakened, giving rise to the manufacturing sector followed by
the rise of the service sector. These two major changes are ascribed to
industrialisation and post-industrialisation. All developing economies are
expected to follow these stages characterised by shifts in the consumer demand
and in labour productivity of the three sectors. Advanced economies such as
those in North America, Western Europe and Japan are currently
post-industrialising; becoming more focused on services and most developing
economies such as those in Africa, Asia and Brazil and are currently
40
industrialising; becoming more focused on industry. However,
data revealed that even in low income countries such as in Kenya, the
contribution of the service sector to the country's Gross Domestic Product
(GDP) is increasing faster than the other sectors of the economy. For instance,
from 2000 to 2010 services growth was about 3.2% compared to manufacturing 1.9%
and manufacturing 1.1%. Growth in services represents nearly two third of the
world's Gross Domestic Product, which amounts to almost 64% of the global GDP
(Service Sector Around the World, 2012).
As the service sector is becoming an important component of
most countries' economies, it is projected to grow at a faster rate in the
future. Service users are currently exposed to a larger range of services and
services are becoming more available to them. Consumers often value services
based on the manner that it has been marketed to them and on the benefits these
services are providing (Londre, 2010:1). Quality service is perceived as the
major cause of customer satisfaction. Hence providing quality service to
customers is vital to build long-term relationships with both consumers and the
organisation. These relationships can lead to increasing profitability and
customer retention (Olusoji, 2009:7).
To be globally competitive, service organisations should
develop knowledge and insight into three major aspects of service such as
services marketing, service quality and customer satisfaction (Naik, 2010:
242).These aspects are consecutively discussed.
3.2. SERVICES MARKETING
3.2.1 Definition of services marketing
With the rapid growth in the service sector, most service
organisations such as insurance, telecommunications and hospitals have
recognised the importance of services marketing to promote the value of their
services to customers to increase their profitability. Organisations are
becoming interested in learning how far this development is reflected within
their marketing curriculum. Increasing organisational profit requires a strong
coordination between the marketing department and customers to provide customer
satisfaction (Verma, 2012:33). The application of services marketing is vital
as it will push and persuade customers to purchase services. Hence, the concept
is often
41
connected to terms such as communication, sales and
advertisements (Kasper, Helsdingen & Gabbott, 2006:76).
From the discussion provided, the definitions of services
marketing can be presented in Table 3.1:
Table 3.1 Definition of services marketing
Definition
|
References
|
Descriptions
|
A
|
Services Marketing (2012)
|
Services marketing relates to
promoting economic activities to
customers. It might involve
selling services such as
health, telecommunications, insurance, education, air travel, electricity and
water to customers.
|
B
|
Jupiter (2011)
|
Services marketing refers to the
process of persuading
prospective customers to
purchase a business service.
Services marketing comprises
the techniques used in the
overall marketing plan of
production, pricing, promotion
and distribution.
|
C
|
Zeithaml & Bitner (2007:22)
|
Services marketing involves
providing services that actually
satisfy the needs, wishes,
whims and the preferences of
present and future customers. To accomplish this mission, an
organisation must select a
target group and address their
needs accordingly.
|
|
42
D
|
Kasper et al. (2006:76)
|
Services marketing refers to a
set of functions such as
communication, advertising,
|
|
|
and delivering service value to
|
|
|
consumers and for managing
|
|
|
customer relationships in order
|
|
|
to increase a firm's profitability.
|
|
From the definitions provided in Table 3.1, services
marketing can be viewed as a subfield of marketing that consists of the
marketing of services by an organisation to its customers.
3.2.2 Generic elements of the definition of services
marketing
From the definitions provided in Table 3.1, some generic
elements of services marketing will now be discussed.
? Promoting customer satisfaction through the
creation, distribution, promotion and pricing of services
Services marketing is first an instrument for promoting
customer satisfaction through the creation, distribution, promotion and pricing
of service. It is a continuous process of convincing potential consumers to buy
an organisation's services (Jupiter, 2011). The core idea is that for a service
organisation to grow, its customers must be satisfied. Happy customers are more
likely to return to the organisation to repeat purchases. Customers spend their
money to acquire services that must satisfy their needs. Such services must
have optimum level of quality, reliability and must be offered to consumers at
the right price and advertised effectively to attract them (Fornell, Rust &
Dekimpe, 2010:29).With the current global competition, services marketing
requirements have considerably changed. As a result, a current effective way to
keep customers satisfied, rarely has longevity. For example, old cassette decks
no longer satisfy the needs of most music listeners, they have been replaced by
compact discs and mp3 music players. They have thus replaced the dominant share
of Samsung`s range. Therefore, services organisations must constantly assess
and address their
43
customers' services needs and be ready to adjust the marketing
of their services accordingly (Grönroos, 2007: 266).
? A tool for managing, identifying and satisfying
customer requirements profitability
Secondly, services marketing can be seen as a tool for
managing, identifying and satisfying customer requirements. It concentrates on
the distinctive features of services and how they can be properly managed in
order to impact both the consumer behaviour and the entire organisation
(Lovelock & Wirtz, 2011:45). Understanding consumers' service needs and
anticipating their requirements are fundamental aspects of the marketing of
services. Service organisations must be aware of market trends and developments
that may have an influence on both consumers' views and the activities of
organisations operating in that specific marketplace. These changes can be
referred to as social, technological, legal and regulatory changes, as well as
political developments and competition in the market. Thus businesses must
offer services, with alternative solutions to consumers' specific needs, in
line with all trends in the market. The competitive nature of the market must
be of a major importance to services marketers. Organisations must make use of
their internal resource base to determine which path to take in order to be
successful. Therefore, an effective marketing of services will rely on the
successful evaluation of customers, the market environment, competition and the
company's internal resources (Zeithaml et al., 2006:8).
? A system that fits the service product to the
customer
Thirdly, services marketing can be regarded as a system which
fits the service product to the customer. It is regarded as an activity that
identifies the service needs and preferences of a target group and addresses
those needs accordingly (Zeithaml & Bitner, 2007:22). For an organisation
to address this issue, it must create a marketing strategy where the goal is to
identify groups of customers with similar needs and develop services to address
those needs. As a result, each population group may then be proposed a
specifically tailored service, according to their specific requirements.
However, for organisations to effectively propose services to customers, they
must focus primarily on the segments of customers they are capable of serving
and who will provide satisfactory returns. The limited resources will not allow
organisations to target all groups in the market. As a result, service
organisations have to select an appropriate
44
service positioning framework to have a competitive advantage
over rivals in the market (Zeithaml et al., 2006:8).
? Services marketing as a set of tools and
activities
Fourthly, services marketing can be perceived as a set of
designed tools, techniques and activities such as pricing, promotion and
distribution of services to prospective customers (Savescu, 2011:39).
This constitutes a major part of marketing since it is the
one to which consumers are exposed. Marketing of services should not only
involve acquiring customers, promotion, pricing, and distribution of services,
but also include keeping and building a solid customer relationship (Temesgen,
Negi & Ketema, 2010:51). Thus, three major levels of the marketing of
services have been identified: recruiting customers, keeping customers and
growing customers. Regarding the recruitment of customers, a service
organisation will develop activities such as the marketing, delivery and
pricing of their service product to persuade prospective customers than the
service provided is better than the competitor's one (Jupiter, 2011).
In order to keep customers, an organisation can develop its
customer contacts during the service delivery process in a way to impact a
customer positively and influence him or her to continuous purchasing. Finally,
to grow customers, an organisation has to sustain a real relationship with a
customer, where the customer feels emotionally attached to the organisation
(Grewal, Chandrashekaran & Citrin, 2010:612).To achieve this, an
organisation has to develop a relational approach when proposing its services.
During this approach the organisation must show the customer its willingness to
take care of him. In addition to providing services, the customer must perceive
it to have a satisfactory outcome-related technical and process-related
functional quality. If the customer is happy with the perceived services, then
he may probably prolong his relationship with the organisation (Grönroos,
2007:270).
3.2.3 The importance of services marketing
Services marketing is fundamental to services organisations;
it refers to the promises made and promises kept to consumers. Good marketing
of services often results in organisations' development. If organisations are
able to innovate their services
45
marketing, then the socio-economic change will arise at a
faster pace (Gilaninia, Almani, Pournaserani & Mousavian, 2011:787). One of
the major boosts to services marketing is technological developments. These
developments offered opportunities to organisations to market and carry out
services in a manner that the consumer's physical presence is no longer a
requirement. For example, Internet technologies have enabled customers to
access services using their computers. This has significantly improved the
traditional way of providing services (Hoffman, Bateson, Wood, & Alaxandra,
2006:15).
The Internet has been used to assist in the service process
such as selling, communicating, making payments and conducting market research.
It is perceived as a marketing channel where most service interactions can be
performed. The Internet has been involved in the service delivery process by
offering help-desk services and support services to customers (Grönroos,
2007:283). Another consequence of information technology development is the
rise in value-added and service quality. This aspect is merely crucial for
organisations which compete by differentiating their products via offering
superior service. New technology developments such as ATMs have enhanced
services in the financial sector by substituting the traditional bank counters.
ATMs are known to providing fast and high quality service to customers (Kasper
et al., 2006:325).
High technology services such as e-commerce in general can be
perceived as time saving for both the service producer and the customer.
Services can be accessed seven days of the week without any requirement for the
consumer to go to the service organisation. An additional advantage is the
creation of the place utility, where services can be accessed from anywhere,
such as by laptop or mobile phone (Kasper et al., 2006:325).Additionally, the
use of technological services can provide a competitive advantage in various
ways. One of the benefits is the substitution of labour, which can
significantly lead to an organisation's cost reductions. This aspect can enable
organisations to become more competitive and to increase profitability (Kasper
et al., 2006:324).
A final observation revealed that technologies used by
service organisations such as banks, hospitals, hotels and communications
services may be less polluting to the environment as opposed to technologies
used in manufacturing organisations which may have a more harmful effect on the
environment (Greenstone & Hanna,
46
2011:10).It is therefore important to note that although
technology development has significantly substituted labour in many service
organisations, most organisations such as hospitals still rely heavily on human
labour to offer services to patients who feel more comfortable interacting with
human beings. In that case the marketing of services relies more on the direct
interactions between patients and the medical personnel (Kapoor, Paul &
Halder, 2012: 11).
Findings suggested that involving patients in the course of
medical care has a significant impact on the medical treatment results. Medical
outcomes no longer depend on medical employees' skills only, but may vary
depending on the degree of patient participation in the process of care. There
is a correlation between patient involvement in the process of care and medical
success. In the current millenium, patients are becoming more aware of quality
service via the Internet. As a result, they may require superior services in
hospitals. This in turn reveals the necessity to foster services marketing in
hospitals (Tan, Benbasat & Cenfetelli, 2013: 87-88). Patient satisfaction
results from quality in health care through health services marketing where
health care institutions can market their offerings to gain more customers and
become more competitive. Services marketing has a greater effect on patient
behaviour than the costs he or she has to endure in hospitals. As a result,
services marketing can portray a positive image of the hospital, which in turn
will allow patients to remain more loyal and refer the facility to other
individuals. Doctors usually disregard the importance of health services
marketing. They usually assume that patient satisfaction merely depends on
their technical expertise. As a result, they often underestimate the economic
benefits of implementing services marketing in hospitals. Health services are
often perceived as a complex mechanism that comprises both the technical
abilities of doctors and their ability to market their services to patients
(Dosen, 2009:2007).
Rohini (2006:69) indicated that patients' perceptions of
service quality are mostly influenced by the ability of medical institutions to
market their services. As a result, medical personnel should be able to
communicate, support, listen to and notify patients about their health
concerns. These service delivery traits are highly rated by patients and
display a positive image of the organisation in the mind of a patient. This in
turn influences patient choice of health service provider.
47
3.3 MANAGING ORGANISATIONS IN A SERVICE
ENVIRONMENT
In order to manage services effectively, it is vital for
services organisations to have an understanding of the different dimensions
involved in a service. The distinguishing elements of services are crucial in
the design of a proper marketing mix for the service organisation. The
identification of these elements was the preoccupation of much earlier research
by Hoffman et al., (2006:26) and conceptual development by Kasper et al.
(2006:76) of services marketing. The different elements are known as
intangibility, inseparability, perishability, heterogeneity, ownership and
service culture (Zeithaml et al., 2006:20). All these elements require the
involvement of employees in delivering the service and refer to the hidden part
of revealing the brand awareness of the organisation (Conradie, 2011:69). Each
of the mentioned elements is briefly discussed next.
3.3.1 Different dimensions when managing an organisation
in a service environment
? Intangibility
Intangibility is the main feature of a service. This implies
that a service cannot be seen, smelled and touched (Grobbelaar, 2006:5). Health
care services result in actions such as surgery, diagnosis, examination and
treatment offered by doctors. These services cannot be seen or touched by the
patient, although the latter may be able to see or touch some tangible aspects
of the service such as medical equipment (Zeithaml et al., 2006:20). However,
the intangible nature of services can present major concerns in a way services
are not easy to display or to communicate to customers (Grobbelaar, 2006:6). As
a result, customers usually use price as a basis for evaluating service quality
(Zeithaml et al., 2006:21).
? Inseparability
Inseparability refers to when services are produced and
consumed at the same time. Customers generally take part in the course of
service delivery and their role is vital in the service production process
(Grobbelaar, 2006:7). However, the nature of
48
interactions between the service provider and the customer can
influence the outcome of the service performance. Service providers are often
perceived as the service itself. Therefore firms should recognise their
important role in service processes (Zeithaml et al., 2006:22).
? Perishability
This aspect of service implies that services cannot be
inventoried, stored or re-used once they are produced (Grobbelaar, 2006:7).
This can present major concerns in the supply and demand for services since
service failures cannot be recovered to balance their demand and supply. As a
result, service marketers must implement strategies to pick up from service
process failures. This forces firms to build more efficient capacities to plan
and manage future demand (Kasper et al., 2006:60).
? Heterogeneity
Services comprise intangible performance mostly delivered by
human being. However, due to the changing nature of people, human performance
will frequently vary. As a result, two services cannot be precisely alike.
Customers often see the service provider as the service itself and therefore,
the service is often perceived as heterogeneous (Grobbelaar, 2006:7).
? Ownership
Since services are produced and consumed at the same time,
they cannot be owned or exchanged by consumers. As a result, the purchase of a
service provides the right to access the service only, and not its ownership.
Customers are usually unsure about the outcomes of a purchased service, and
also whether the service will or will not adequately satisfy their needs
(Conradie, 2011:72). Since services are perishable, they cannot be returned.
This suggests that firms should foster a culture of service excellence to
ensure that quality service is provided to customers (Kasper et al.,
2006:61).
49
? Service culture
Service culture is influenced by the value and culture of an
organisation that guides service employee behaviours, which is in turn
associated to the organisation's outcomes (Webster & White, 2009:692).Thus,
organisational culture is important as it has a large impact on service
processes. Given the fact that services are heterogeneous and intangibles, it
is not easy for customers to assess the services received as opposed to goods.
Customers often take into account other aspects of interaction with service
employees such as their behaviour. Employees' behaviour results from an
organisational culture (Mosley, 2007).
Service culture usually builds up over time and is relevant
when interest in customers is the most critical value in the organisation
(Conradie, 2011:72).However, sustaining a service culture in an organisation
does not imply that other values are no longer important. Grönroos
(2007:418) regards service culture as a culture where providing high-quality
service to customers must be the core value of an organisation. As a result,
all employees within organisations must be service oriented. This means that
service employees must share common values and attitudes so to improve and
provide excellent services to customers (Grönroos, 2007:419).
Successful services organisations must have an understanding
of the characteristics of services. The distinguishing features of services are
important in the design of a proper services marketing mix to address the needs
of customers and to remain competitive (Du Plessis, 2010:198). An understanding
of the services marketing mix will be provided in the following discussion.
3.3.2 The services marketing mix
Developing a successful marketing plan is vital to maintain a
customer orientation. The marketing mix focuses on choosing the right marketing
mix elements. It involves combining ideas, concepts and features in order to
better address customers' needs in a given market. The marketing mix is
composed of four major aspects such as product, price, promotion and place.
Unlike the product marketing mix, services marketing is
50
characterised by three additional elements such as people,
process and physical evidence. These aspects constitute a services marketing
blueprint design (Conradie, 2011:72).
Each of the elements is briefly described next.
? Product
The services marketing product mix is usually intangible,
which means it cannot be measured. Education, tourism and the health care
industry can be perceived as good examples of services marketing mix. Major
characteristics of these service products are that they are heterogeneous,
perishable and cannot be owned (Hu, 2011:61). In general, a careful design of a
service blueprinting is a prerequisite to define the service product. For
example, a fast-food blueprint is vital prior to establishing the fast-food
business. The service blueprint will describe how the product referred to as
the fast-food business will be (Bhasin, 2011).
? Place
Place refers to where the organisation is going to sell its
services and where they are going to be implemented (Conradie, 2011:148). For
example, a good place to establish a petrol station will be in the urban area.
Therefore, an area with low traffic will be regarded as inappropriate for a
petrol station. Additionally, a software business will be best suited in a
business hub with various organisations around, rather than being isolated in a
rural area (Lings & Greenley, 2009:44).
? Promotion
Promotion of services is vital for organisations to survive
in the competitive world. Services are easily imitated; therefore organisations
have to differentiate and distinguish themselves from the rest through their
brand. Thus promotion has become a significant component of the services
marketing mix (Hu, 2011:61). IT organisations, hospitals, hotels and banks set
themselves above the rest by promoting their services to customers (Kasper et
al., 2006:465).
? Pricing
51
Service pricing is quite different from product pricing as it
takes into account labour, material cost and overhead costs. For instance, a
fast-food owner may price his food based on the pleasant ambience the facility
may provide to people and the band customers have for the music. Thus, services
pricing can be made of all the costs involved to mark up the final service
price (Pomering, Noble & Johnson, and 2011:961).
? People
People constitute an important constituent of services
marketing as they define a service. For instance, nurses and medical people
define health services; bank employees will define the type of financial
services provided to customers. Thus people employed in services can affect
positively or negatively on an organisation (Pomering, Noble & Johnson,
2011:962-963). Various organisations are getting their personnel trained in
interpersonal skills and customer service to ensure better service delivery and
customer satisfaction. Nowadays, most organisations are getting accreditation
in terms of showing that their personnel are better than the rest (Bhasin,
2011).
? Process
Process refers to the manner in which service is provided to
the final consumer. For examples, two medical services providers: Milpark and
Garden City Clinic hospital thrive on their fast service and the reason they
can do that is based on their confidence on their processes. Additionally, the
demand for their services is such that they have to provide quality service to
their patients. Therefore, the service process of an organisation is vital
(Prouse, 2011). It is also part of the service blueprint, in which prior to
establishing the service, an organisation has to identify what should be the
process of the service product reaching the final consumer (Kasper et al.,
2006:465).
? Physical evidence
Physical evidence refers to the final component in the
services marketing mix. Since services are intangible in nature, physical
evidence of services is vital to create a better consumer experience with the
service provided (Lovelock et al., 2009:24). A patient is more likely to choose
a private hospital with air conditioner, excellent patient care, advanced
medical equipment and a prompt service delivery system than a government
hospital. Thus, physical evidence is crucial in the services marketing mix,
since it acts as a service differentiator (Bhasin, 2011).
52
3.4 THE THREE LEGS OF SERVICES MARKETING
Interaction between the consumer and the service provider is
vital in services. These human to human interactions form variability in the
service provision for every individual consumer (Olusoji, 2009:27). A structure
known as the services marketing triangle highlights the value of people in the
ability of organisations to ensure that promises are kept and achieved in
building relationships. The services marketing triangle helps marketers in
dealing with issues such as understanding consumers' needs and expectations of
services, enhancing the value of services to consumers, and ensuring that
promises made to consumers are kept (Conradie, 2011:76).
3.4.1 The services marketing triangle
Service triangle is a method used by organisations to
highlight the importance of employees and organisations in keeping their
promises and building a solid customer relationship. The triangle focuses on
three major elements namely the organisation's management, customers and
employees. Between each of the three elements of the triangle, there are
various marketing processes such as external, interactive and internal
marketing. These processes have to be conducted properly for service processes
to be efficient and to develop and keep solid relationships with the internal
and external customers (Angelis, De Lima & Siraliova, 2010:10).
Figure 3.1: Services marketing triangle
Internal marketing

Organisation management
External marketing
(Enabling the promise) (Making the promise)
Employees Customers
Interactive marketing Delivering the promise
53
Source: Zeithaml et al. (2006:23).
From Figure 3.1, the three legs of the services marketing
triangle can be explained as follows:
? External marketing
External marketing refers to the service promises made by
organisations to customers. It includes service offerings and the way in which
they will be carried out. External communication is vital to building
customers' expectations, since expectations are influenced by an organisation's
direct and indirect marketing message (Kasper et al., 2006:79).Research
suggested that many organisations have been investing more in marketing
activities such as sales and promotion. This has enabled organisations to
obtain and retain customers. However, investing in marketing becomes
problematic when the cost associated with promoting a product or service is
higher than the profit generated. Thus, it is vital to focus on efficiency and
productivity of marketing department within organisations (Grönroos,
2007:267). A successful coordination of internal and external marketing
communication can enhance marketing efficiency and ensure higher service
delivery to customers (Vrontis, Thrassou & Zin, 2010:26; Zeithaml et al.,
2006:496).
For many organisations, the most critical aspects of managing
brand image involves coordinating all the external communication channels which
send information to potential customers (Lings & Greenley, 2009:44).
However, managing all external communication vehicles has become a difficult
task. In addition to the traditional methods of communication such as
advertising, company website, sales promotion, direct marketing, personal
selling proliferation and public relations, new forms of marketing medias such
as mobile phones, newspapers, magazines, blogs, Internet, television and radio
are currently on the spot. These new medias have made the coordination of the
organisation's messages to customers difficult. Therefore, for organisations to
attract more customers, marketers have to properly control the timing, creating
appeals and placement of all the external communication vehicles (Zeithaml e
al., 2006: 497).
? Internal marketing
54
Internal marketing acknowledges the importance of employees in
delivering services in organisations. By treating employees like internal
customers, businesses can achieve high employee satisfaction and productivity.
Satisfied workers are more likely to become more customer-conscious and deliver
quality service to external customers (Lings & Greenley, 2009:44). Internal
marketing not only regards employees as internal customers, it also encourages
them to develop a positive behaviour towards services delivery. Additionally,
internal marketing focuses on human resource management where the aim is to
recruit, train, mobilise, support, motivate and manage all workers within an
organisation. This vision can enable an organisation to improve the service
strategy for outside customers and internal employees (Shiu & Yu,
2010:796).
? Interactive marketing
Interactive marketing refers to providing excellent services to
customers and keeping
the promises made to them. Interactive marketing enables
contacts between the
service provider and the service user. It gives the
opportunity topeople and companies to interact directly, irrespective of time
and distance (Kasper et al., 2006:79). Interactive marketing communication is
that area of marketing which involves a change of an organisations' ideology
where customers are perceived as partners. It is a strategy that allows
customer to provide immediate feedback by means of various forms of
communication such as audio, video text, interactive television and virtual
reality (Vlasic & Kesic, 2007:111).
Service quality is an important indicator of effectiveness of
both employees and organisations in keeping their customers satisfied (Siddiqui
& Sharma, 2010:222). It is fundamental to all three legs discussed, since
quality results in increasing satisfaction and performance of all parties
involved in services. Service quality is an integral component of both internal
and external customers on their evaluation of a service. It is an essential
aspect to ensure customer satisfaction (Jun & Cai, 2010: 2006). The concept
of service quality will be discussed more comprehensively next.
3.5 SERVICE QUALITY
Service quality is often described as the consumers'
perceptions of the service received. It is a subjective impression of the
relative inferiority or superiority of a service provider
55
and its services. Service quality is usually considered
comparable to the consumer's attitude with regard to the organisation (Siddiqui
& Sharma, 2010:222).
3.5.1 Defining service quality
Achieving customer satisfaction has become a major concern in
most service organisations through proving service quality (Irani, 2008:33). A
customer's satisfaction level is influenced by his experience with services
provided and by comparing that experience with the type of service which was
expected. Studies revealed that service quality and customer satisfaction are
two major constituents of customers acquisition and retention (Hossain &
Leo, 2009:338).
Experts believe that successful organisations are those which
remain in the mind of their customers. This can be achievable if they provide
excellent services. Thus service quality has become an essential tool to assess
organisational performance and to promote customer satisfaction (Rezaei et al.,
2011:483).
Various definitions of services quality are presented in Table
3.2:
Table 3.2: Definition of service quality
Definition
|
References
|
Descriptions
|
A
|
Rezaei et al. (2011:485)
|
Service quality is the delivery of excellent or superior
services relative to customer expectations. There is a positive correlation
between service quality and customer satisfaction. As a result, superior
service often leads to increase in customer satisfaction.
|
B
|
Mohammad and Alhamadani (2011:61)
|
Service quality is perceived as an intangible economic
activity that provides psychological benefits to the customer. It's a type of
service provided which meets the external customer's needs.
|
C
|
Siddiqui and Sharma
|
Service quality refers to the
|
|
56
|
(2010:222)
|
service user's assessment of the service he or she has received.
It is a relative evaluation of the superiority or inferiority of a service
provider and its services, and it determines the customer's overall attitude
towards the organisation.
|
D
|
Kasper et al. (2006:178)
|
Service quality refers to the extent to which the service
product successfully serves the purpose of the user during the usage. This
implies that happy customers are more likely to repeat purchases and remain
loyal to the firm.
|
|
From the definitions provided in Table 3.2, service quality
can be viewed as an evaluation of how well a delivered service matches the
customer's expectations.
3.5.2 Generic elements of service quality
From the definitions provided in Table 3.2, some generic
elements of services marketing will now be discussed.
? Service quality as a transcendent-based
quality
According to this approach, service quality is often
described based on individual rather than shared experience. This is often
perceived as epiphenomenon, where a person can understand what something is,
but is not able to describe it. He or she usually makes use of comparison or
reference to something (a comparator) (Benlian, Koufaris & Hess, 2012: 88).
For instance, a person may say that the service experience of MTN is better
than the Vodacom one without being able to tell why. This approach shows that
service quality cannot be described accurately, but only through comparison of
one service experience to another. It is then referred to as transcendent
(Kasper et al., 2006:178).
57
? Service quality is user-based quality
This element highlights the degree to which services
successfully fit the customer's purpose during usage. From this point of view,
service quality is simply determined by the service user and is very
subjective, since every customer has a different approach to quality
(Bogomolova, 2011:793). The problem is that this approach emphasises merely on
perceived quality that is not a very reliable indicator of the actual service
quality. This can be costly for an organisation that wants to please all its
customers, but at the same time cannot provide different types of services in
response to different types of customer services quality requirements. To
resolve this problem, service organisations can provide customised services to
their customers. Customisations can be used to ensure individualised service
quality and can be a low cost strategy for an organisation. An example of
customisation is the Inter-continental five star hotel which has a large range
of guest rooms and services customised according to each different class of
clients (Grönroos, 2007:73).
? Service quality is value-based approach
In this approach, quality exceeds users' expectations of
service. This simply means that the value-based view regards service quality as
a function of customer benefit relative to cost (Rust & Huang, 2012:47). In
other words, this approach evaluates service quality as the difference between
customers' expenses to acquire the service and the actual satisfaction he or
she receives from it. The perceived value of service quality can result from a
complex evaluation of both the service and service user's attributes. In this
regard service quality can sometimes become ambiguous. In airline travel, all
passengers are heading to the same destination at the same time, but the
service cost will differ according to the different class of travel. Or, in
various states, a customer`s bank charges will be higher if he is served by a
bank employee rather than if he uses the Internet or an ATM machine (Kasper et
al., 2006:178).
3.5.3 The importance of service quality
58
Service quality is fundamental for organisational success and
survival. It is vital in most service organisations. Fostering service quality
is a way services organisations can distinguish themselves from competitors and
increase their market share. Researches demonstrated that offering service
quality can retain customers as well as attracting new ones. The cost of
marketing to old customers is significantly reduced compared to if
organisations had to market to new customers. Once customers become familiar
with the organisation, they develop trust and their level of risk is
significantly diminished. This implies that they are more likely to remain
faithful to the organisation (Hoffman et al., 2009:400).
Providing quality goods has been a long-time ideology of the
good manufacturing industry. It has led to increasing market share, customer
satisfaction level and improving a firm's efficiency. The quality perspective
in the good manufacturing firms focuses primarily on improving the quality of
goods through eliminating defective products. This philosophy is enforced by
careful monitoring and verification of all finished goods before they are
delivered to the final consumer. The early development of the concept focuses
on ensuring quality during the manufacturing procedure so as to limit the
number of faulty products to zero. Recent developments regard quality as
providing the right product to the right customer and at the right time, hence
expanding quality beyond the good itself, and using internal as well as
external assessments to evaluate the firm's overall quality (Golder, Mitra
& Moorman, 2012:2).
Service organisations have a different quality system
framework. Service quality relies on the customer`s involvement in the
production and quality control process. Additionally, achieving service quality
must be a daily continuous effort of all employees involved in the management
and production of services (Hoffman et al., 2009:400).
3.5.4 The different elements of service
quality
A major concern to assess service quality is to identify what
elements customers utilise to evaluate quality. The SERVQUAL model was develop
to provide a more comprehensive understanding of service quality. The model
highlights five major attributes of service quality such as reliability,
assurance, tangibility, empathy and responsiveness that have become dominant in
service quality research (Kasper et al.,
59
2006: 189).These dimensions have been successfully used to
assess service quality not only in service industries, but in hospital settings
as well (Yesilada & Direktor, 2010).
From the previous discussion, each element of service quality
will now be reviewed:
? Reliability: This refers to the ability to provide the
service correctly and dependably. In the hospital industry, it is the degree to
which the consistency of service promises such as keeping appointment times,
completing duties on time and respecting all promises made to patients are met
(Basheer, Al-Alak & Alnaser, 2012:157).
? Assurance: This dimension encompasses competence, courtesy,
credibility and security. This element involves training of employees to
acquire knowledge of the service delivery process and customer relationship.
This is a vital aspect to provide excellent services and the perception that
the service provider is competent and not going to harm anyone. This can also
build trust in the customer's mind (Meng, Summey, Herndon & Kwong,
2009:775).
? Tangibles: This refers to the tangible aspects of service
such as the appearance of physical facilities, equipment and personnel. These
elements have a significant influence on the perceived service quality. In
hospitals for instance, cleanliness of premises, staff appearance, decor,
computers and medical equipment can all have a positive or negative impact on
the patient's perceptions of service quality (Kasper et al., 2006:189).
? Empathy: This element includes communication, access and
understanding. It focuses on the communication aspect between the service
provider and the recipient of service. In hospitals, empathy is reflected in
the ability of medical personnel to care for their patients (Basheer et al.,
2012:157).
? Responsiveness: This refers to the willingness to help
customers. Service providers must be willing to respond to individual customer
needs such as making sure that customers remain involved and detailing delivery
times (Kasper et al., 2006:190).
3.5.5 Failure gaps in service quality
It is often difficult to investigate and apply service
quality in organisations. Firstly, service quality perceptions rely on the
repetitive comparison of the service user's expectations about a specific
service. This means that if a service does not repetitively
match the user's expectations, it will be considered as poor,
no matter how good the service is. Secondly, contrary to good products where
users only assess the final good, service users assess both the process of the
service and its effect. A person having a haircut will assess quality based not
only on his perceptions of the hairstyle, but also on whether the hairdresser
is welcoming and skilled. Studies revealed that service quality is evaluated
from gaps between expectations and perceptions on the side of management,
employees and service encounters (Hoffman et al., 2009:403).
The following figure provides an overview of the different
gaps that may exist in service quality.
Figure 3.2: Service quality gap model
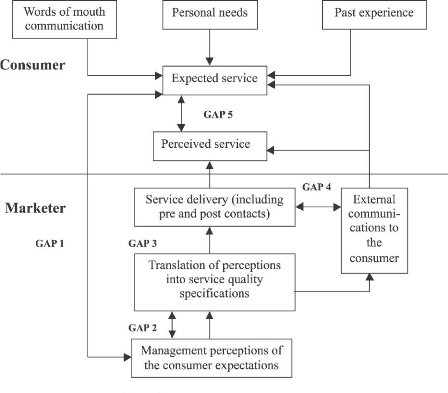
Source: Rajasekhar, Muninarayanappa and Reddy (2009: 220)
60
61
? Gap 1
It refers to the difference between the customer expectations
of service and the management perceptions of the consumer expectations. Often,
managers think they know what their customers want, while in fact they are just
speculating. In the medical industry, this may lead to the wrong services being
offered to patients and dissatisfaction of patients with the service provided.
Therefore, minutely detailed knowledge of what patients' needs are will be a
prerequisite to close this gap (Holder, 2008:46).
? Gap 2
It is the difference between management's perception of
customer expectations and the current standards set for service delivery. To
close this gap, when setting standards in the hospitals for instance, managers
should identify all key aspects of interactions between employees and patients.
Detail standards can be written such as the way employees should operate and
behave at each level of the hospital (Hoffman et al., 2009:404).
? Gap 3
It consists of the difference between the current performance
of a service and the standard set by the organisation's management. In the
medical industry, this gap results from the willingness of medical staff to
offer the service according to specifications. The questions can be asked if
medical staff wear their uniform before performing the service, and if they
thank the patient when the service is completed (Zeithaml et al., 2006:38).
? Gap 4
It is the difference between the promised service of the
organisation through its external communication channel and the service that is
actually delivered to customers. If an organisation advertises a particular
service to customers and that customer receives a different type of service,
then the communication gap will widen. To close this gap, managers should work
with all departments to make sure that promises made on the advertisements are
fulfilled (Kasper et al., 2006:195).
62
? Gap 5
It refers to the difference between what service users expect
from a service and the actual perceived service. Customers' expectation is a
subjective evaluation of a service. Patients often have different expectations,
therefore they make different assessments of the service provided, which can
lead to dissatisfaction (Holder, 2008:45).
Service quality is fundamental to every organisation.
Organisations that offer better service quality increase demand by increasing
customer acquisition, customer retention, and consumer loyalty (Liu &
Homburg, 2007). There has been a positive correlation between the service
quality provided in organisations and customer satisfaction. This assumption
suggests a close relationship between service quality and customer satisfaction
(Rust & Huang, 2012:49).The concept of service quality will be discussed
more comprehensively next.
3.6 CUSTOMER SATISFACTION
Customer satisfaction is perceived to have an impact on the
choices and purchasing behaviour of consumers. Satisfied customers are more
likely to increase spending compared to those who are dissatisfied with the
service provided. Consequently, satisfied customers can significantly increase
an organisation's profit. Evaluating customer satisfaction has become a central
philosophy among most organisations (Fornell et al., 2010:29).
3.6.1 Defining customer satisfaction
Customer satisfaction has become a major concern and focus in
marketing. Research has shown that satisfaction surveys have been widely used
in various organisations to evaluate service quality. Customer satisfaction has
an effect on the profitability of nearly every organisation. When customers are
satisfied with services, they will more likely tell other individuals. However,
a lack of customer satisfaction has a negative effect on the bottom line.
Customer satisfaction is an asset that should be monitored and managed just
like any physical asset (Bodet & Assolant, 2011:783). Most experts believe
that the surest way to success is to make customer happy. Improving
satisfaction will result in increased customer loyalty and the financial
benefits typically associated with more loyal customers (Forrest et al., 2011:
199).
63
For service organisations, customer satisfaction assessment has
become a major tool to measure organisational performance (Rezaei et al.,
2011:483).
Various definitions of customer satisfaction are presented in
Table 3.3.
Table 3.3: Definition of customer
satisfaction
Definition
|
References
|
Descriptions
|
A
|
Hill, Roche and Allen (2012:18)
|
Customer satisfaction is the discrepancy between customer
expectations and perceptions of the current service provided.
|
B
|
Grigoroudis and Siskos (2012:1)
|
Satisfaction is regarded as
a customer's feeling that
he
or she is being well treated.
|
C
|
Hoffman et al.(2009:369)
|
Satisfaction is a function of expectations that the customer
believes he should receive. Dissatisfaction occurs when the actual outcome is
different from the standard expectation.
|
D
|
Olusoji (2009:12)
|
Satisfaction refers to the consumer's fulfilment response. It is
the subjective evaluation that a service offers a pleasurable degree of
consumption-related fulfilment.
|
|
3.6.2 Satisfaction with care between doctors and
nurses
In health care settings, research has indicated that patients
tend to be more satisfied with nurses care compared to doctors. However, this
does not mean that patients
64
preferred. Patient preferences between doctors and nurses may
relate to various aspects determining satisfaction with doctors' services and
nurses' services. In general, patient satisfaction may arise from the
reliability and responsiveness of doctors in terms of the technical or medical
aspect of care compared to nurses. Such aspects may include medical treatment,
discussing physical complaints, information about the sicknesses and diagnosis
(Laurant et al., 2008:2695). However, patient preference for nursing
practitioners often relates to the assurance and empathy of nurses in terms of
the amount of attention provided to patients, reassurance, and information
about dealing with the disease (Zhang, Liu & Ren, 2013:219).
3.6.3 The generic elements to customer
satisfaction
From the definitions provided in Table 3.3, some generic
elements of services marketing will be discussed next.
? Customer satisfaction seen as an expectancy
disconfirmation model
Customers use the disconfirmation paradigm to compare their
expectations with their perceptions of service. However, if their expectations
coincide with their perceptions, it is said to be confirmed expectations, thus
leading to customer satisfaction. If customer expectations differ from
perceptions of services, then it is said to be disconfirmed expectations
(Cockalo, Djordjevic & Sajfert, 2011:807). There are two categories of
disconfirmations: positive and negative disconfirmation (Hoffman et al.,
2009:369).
? Customer satisfaction as a negative
disconfirmation
Negative disconfirmation occurs when the customer perception
is lower than what was expected. In that case, it will lead to customer
dissatisfaction with the service provided. This may lead to bad word-of-mouth
publicity and a decrease in customer loyalty to the organisation (Orsingher,
Marzocchi, & Valentini, 2011:731).
? Customer satisfaction as a positive
disconfirmation
A positive disconfirmation occurs when the customers'
perceptions go beyond their expectations of services provided. This results in
customer satisfaction. Customers are
65
more likely to refer the organisation to other individuals and
more willing to repeat purchases (Hoffman et al., 2009:369).
3.6.4 Types of customer expectations and the zone of
tolerance
Expectations are seen as optimum levels against which present
and future service encounters are compared. Expectations of service are often
different from present service experience. Research has suggested at least
three different categories of expectations such as predicted service, desired
service and adequate service (Pradhan & Roy, 2011:79).
Predicted service is a probability expectation which relates
to the level of service that service users believe is most likely to encounter.
Hospital patients tend to return to the same medical facility over time.
Patients become used to dealing with the same medical personnel and, over time,
begin to predict certain performance levels. As a result, patient satisfaction
evaluations increase by comparing predicted service to perceived service
experienced (Grobbelaar, 2006:8). Desired service is an ideal expectation which
refers to what service users actually desire, compared with predicted service,
which is likely to happen. However, in most cases, desired service leads to
higher expectation than predicted service. For instance, a patient desired
service would comprise that he receives not only his predicted service, but
that the medical staff call him by his first name and warmly greet him as he
walks into the medical facility (Hoffman et al., 2009:388).
Adequate service is a minimum tolerable expectation and
refers to the level of service a service user is prepared to accept. This type
of expectation relies on experiences or norms which develop over time. Most
people have received medical services from various different hospitals. Through
these experiences, norms develop that patients expect to exist. Therefore,
medical services which fall below expected norms will fall below adequate
service expectations (Grobbelaar, 2006:8).
Services are known to be heterogeneous, and as a result will
differ across employees and service organisations. The degree to which
customers are willing to accept these differences is called zone of tolerance,
which is the difference between desired service
66
and adequate service. The zone of tolerance increases and
decreases among customers depending on service quality, price and the
conditions in which the service is provided. If service provided expands
outside the zone of tolerance (at the desired service), then customers are more
likely to be happy with the service. On the other hand, if service goes below
adequate service, then customers will more likely be dissatisfied with service
(Ince & Bowen, 2011:1772).
3.6.5 Factors influencing service
expectations
Satisfaction relates to the post-decision assessment of a
service. Such assessments lead to repeated choice and thus impact on an
organisation's long-term profitability. Satisfaction is closely connected to
expectations. Expectations refer to predictions of the future, an emphasis of
which can range from broad beliefs to particular product specifications. In
other words, expectations refer to the customers' predictions about how they
will be able to match their choices when exposed to a different set of choices.
A discussion of the factors influencing service expectations are presented
below (Diehl & Poynor, 2010: 313).
3.6.5.1 Desired and predicted service
Desired service expectations are built around six major
factors influencing service expectations such as personal aspects, customers'
personal needs, explicit service promises, word-of-mouth communications and
past experience. Personal aspects develop over time and enhance a customer's
sensitivity regarding how service should be offered (Tsai, Hsu & Lin,
2011:217). This factor comprises two categories; the customer's derived
expectations and personal views of services (Haseki, 2013: 42-43). Derived
expectations are obtained from the expectations of other individuals. For
example, if your manager requests you to hire someone to perform a specific
task in an organisation, your expectations of the one performing the task will
most likely be higher compared to if the person was hired on your own
initiative. In order to please your manager, your sensitivity to quality
service is high. Also, personal views of services refer to customers'
sensitivity regarding the way in which services should be provided. This
implies that customers often desire to be treated in the way they believe they
treat their customers (Heitzler, Asbury & Kusner, 2008:188).Customers'
personal needs imply that some customers are more demanding than others in
terms of service quality.
67
For example, some patients may be interested in both acquiring
excellent medical services and the quality of the tangible aspects of services
such as staff uniforms, medical equipment and toilets. Other individuals may
simply be looking for a proper medical service delivery. Thus, managing a
service organisation can become quite complex (Mitra & Fay, 2010).
Explicit service promises include the organisation's
advertising, personal selling and other forms of communication. In this aspect,
customers assess service based on several sources of communication available.
Often, the more ambiguous the service, the more customers rely on the
organisation's advertising when shaping expectations (Chebat, Sirgy &
Grzeskowiak, 2010). If an organisation promotes clean and attracting rooms,
customers will expect the rooms to be exactly as advertised. Implicit service
promises encompass the tangibles surrounding the service and the price of the
service. If the service price rises, customers will expect higher quality
service in return. Similarly, if tangibles surrounding a service are lush, then
customers will see it as a sign of quality (Hoffman et al., 2009:391).
Word-of-mouth communications are usually entrusted by
customers as they believe in information from people who have been through the
service experience (Berndt & Brink, 2008:56). This type of information can
be provided by family and friends (Kaura & Datta, 2012:66). Past experience
is an assessment of service based on a comparison of the actual service
encounter, and other encounters with the same provider, other providers in the
same industry, and other providers in other industries. Patients evaluate
medical service based on their past experience in other hospitals with other
medical facilities (Hoffman et al., 2009:391).
3.6.5.2 Adequate service
It refers to the level of service a customer is prepared to
accept and is constituted of five factors namely transitory service
intensifiers, perceived service alternatives, customer self-perceived service
roles, situation factors and predicted service. Transitory service intensifiers
are short-term factors which increase the customer sensitivity to service.
Patients are usually prepared to wait for their turn to go to the doctor's
office. However, in emergency situations they become less patient and expect to
receive superior service
68
in a short period of time. As a result, their level of
adequate service rises, and the zone of tolerance narrows (Hill et al.,
2012:17).
The level of adequate service can also be influenced by
customers' perception of service alternatives. Customers who think that they
can receive similar services elsewhere and / or that they can supply the
service themselves, have higher expectations of adequate service compared to
those who think they cannot obtain similar service elsewhere (Babin &
James, 2010). In a self-perceived service role, customers are often seen as
part of the service delivery process. As a result, they can influence the
outcome of the service. However, when their self-perceived role in service is
high or when they believe their role in the service delivery process is
important, their expectations of adequate levels of service rise considerably
and the zone of tolerance decreases (Siu, Zhang & Yau, 2013:675-676).
In situational factors beyond the control of the service
provider, such as if electricity goes out in a restaurant, customers understand
that the problem is beyond the control of the restaurant owner, therefore they
are likely to be more tolerant. Then, adequate service expectations decrease
and the zone of tolerance will increase (Berndt & Brink, 2008:57-58).
Predicted service is the level of service that customers predict to receive. It
is the last aspect influencing adequate service. It refers to all service
promises that organisations make to customers ranging from word-of-mouth
communication to advertisements. Taking these aspects into account, customers
make judgments according to predicted services and set adequate service
expectations accordingly (Berndt & Brink, 2008:56).
3.6.6 The link between expectations, customer
satisfaction and service quality
When assessing service experience, customers always make a
comparison between three categories of expectations such as predicted service,
adequate service and desired service to the perceived service provided.
Customer satisfaction is evaluated by comparing predicted service and perceived
service. Perceived service adequacy that complies with adequate service and
perceived service, and perceived service superiority, that desired service and
perceived service, are measures of service quality (Hill et al., 2012:18).
Kasper et al. (2006:105) argued that expectations are a major determinant of
satisfaction, and expectations may be influenced by various factors such
69
as cultural, race, gender, education, socioeconomic,
geographical, education and age differences. Younger patients are more
demanding with regard to service quality provided in hospital settings compared
to older patients. Additionally, Olusoji (2009:23) viewed that patients with
higher educational level, were more informed with regard to medical service
quality and therefore were prone to expect better care compared to those with
low educational background.
There is other evidence that expectations may differ
according to knowledge and prior experience. This means that expectations are
likely to change with accumulating experience (Pradhan & Roy, 2011:79).
Zeithaml and Bitner (2007:60), for instance, observed that enhancing quality of
medical services raises expectations. From this observation, an increased level
of expectations of quality among patients may gradually be associated with a
low level of satisfaction.
Other writers such as Youl Ha (2006:137) suggested customer
satisfaction as being central to an organisation's profit, and that
satisfaction is linked to a customer's perception of service provided and the
extent to which these services match the customer's expectations.
Bick, Abratt and Möller (2010:14) noted that there is a
direct relationship between customers' expectations, service quality,
satisfaction and increase of purchase. Raboka (2006:128) suggested that
services that match or go above customers' expectations will result in customer
satisfaction, and services that go below customers' expectations will lead to
customers' dissatisfaction with services provided. Furthermore, satisfied
customers are more likely to remain loyal to the organisation and increase
purchase. Youl Ha (2006: 137) observed that customers' choice of services
provided can be a complicated mental process and may differ from one period to
another. As a result, organisations should continuously measure customers'
perceptions of services if they strive to remain competitive.
3.7 CONCLUSION
In this chapter the focus was on the concepts of services
marketing, service quality and customer satisfaction in perspective. The
definitions, generic elements and importance of services marketing, service
quality and customer satisfaction have been highlighted. Additionally, a
discussion on the relationship between expectations, customer
satisfaction and service quality has been included in the
chapter. Recent studies suggested that organisations have shown major concerns
about services marketing, quality and satisfaction. It is evident that
improving marketing of services and quality in an organisation may possibly
increase the levels of customer loyalty, profits and market share (Olusoji,
2009:7).
Chapter 4 will focus on the methodology used to conduct the
survey. A comprehensive focus will be provided on the scope of the study, the
sampling method, organisation of the survey, validity and reliability of the
questionnaire, the data gathering technique, data analyses, as well as the
reliability of the results.
70
CHAPTER FOUR: RESEARCH METHODOLOGY
71
4.1 INTRODUCTION
Any business hoping to attract more customers and to keep
them happy must focus on service quality. Service quality can be used as a
strategy to attract consumers if companies can understand their behaviour. This
understanding is made possible through intensive research (Rezaei et al.,
2011:483). Research problems involve proper planning to find solutions.
Research involves efficient gathering, evaluation and explanation of
information for decision-making. This can be done through scientifically
accepted methods. Since research is perceived to be time consuming, researchers
must be methodical when collecting data that they must evaluate for the
research at hand. The analysis and explanation of data depend on the
researcher's own experience and his understanding of the subject of interest
(Naidoo, 2008:73).
This chapter offers a theoretical illustration of the
research process. It emphasises on the population, the chosen sample, the
questionnaire design, the method of data gathering, as well as data analysis.
The framework of the research is based on the different stages in the research
process as illustrated in Figure 4.1.
4.2 THE RESEARCH PROCESS
A proper recognised research process often involves the
different stages as illustrated in Figure 4.1. However, it is vital to know the
interdependency of each stage involved in the process. This enables better
understanding of the various stages in the research process as discussed
next.
72
Figure 4.1: Stages in the research process

Source: Cant, Gerber-Nel and Kotze (2005:39)
4.2.1 Step 1: Identify and formulate the problem or
opportunity
The first stage while conducting research is to identify and
formulate the problem (Malhotra, 2007:10). The problem statement of this
research was conducted in Chapter One, section 1.3, and is repeated for ease of
reference.
The government of Gabon has improved the health care system
in the country through the provision of health care infrastructures, and by
increasing the number of government hospitals in the country in order to allow
more patients to have access to medical care services. However, there seems to
have been a shift of patients from government health care hospitals to the
newly established military hospital. The new facility has attracted a large
number of patients from various parts of the country. There is no clear
understanding of why patients have shifted towards the military hospital.
73
During a telephone interview conducted on 6 March 2012, a
medical personnel at the military hospital stated that patients seem to have
been dissatisfied with services provided in the government hospitals. Moreover,
the link between services delivery at the military hospital in Gabon and
patient satisfaction has not been yet investigated before. Hence, these two
features need to be investigated as the study could offer a way to promoting
effectiveness and profitability in medical institutions.
4.2.2 Step 2: Determine the research objectives
This stage involves building a theoretical framework,
research questions and hypotheses, and recognising the information required for
the research (Malhotra, 2007:10; Hair, Bush & Ortinau, 2006:55). The aim of
this study is supported by different aspects as discussed in section 1.5 of
Chapter One. Various hypotheses were formulated in section 1.5.3 of Chapter One
to help determining the parameters of the research. The primary objective of
this research is to establish the perceptions of patients regarding the service
quality received from doctors and nurses. More particularly, how they rate
doctors and nurses on the service quality dimensions. The secondary objectives
aim:
· To determine how patients rate the reliability
of doctors and nurses.
· To establish how patients rate the responsiveness
of doctors and nurses.
· To determine how patients rate the assurance of
doctors and nurses.
· To establish how patients rate the empathy of
doctors and nurses.
· To establish if there is a difference in how patients
rate doctors and nurses on the service quality dimensions.
· To establish the perception of patients regarding the
tangible aspects of a military hospital in Gabon.
4.2.3 Step 3: Research design
A research design represents a framework of how a research
study has to be conducted. However, one needs to differentiate between two
types of research namely, quantitative and qualitative research. Qualitative
research concentrates on words, stories, signs, visual representations,
observations and interpretations of social facts. Quantitative research makes
use of numbers; it aims at explaining some facts with the
74
use of numbers Holder (2008:5). For the purpose of this
research, the researcher made use of a quantitative method.
4.2.3.1 Quantitative research
This research focused on a quantitative study. The motive for
choosing a quantitative study is that it is simple to explain the results in
simple conclusions. A quantitative study includes gathering primary data from
large numbers of respondents with the goal to project the result to a broader
population. This research type quantified data using statistical analysis
(Zikmund & Babin, 2007:83).
A quantitative method was utilised for the purpose of this
research to gather responses from respondents. The quantitative technique is
suitable when the population is large and objectivity is extremely important
(Rootman, 2006:111). Quantitative data was collected from respondents using
self-administered questionnaires.
4.2.3.2 Descriptive research
A descriptive study provides a deep description of the
research problem. It aims at finding answers to questions of who, what, when,
where and how. Descriptive research focuses on precision, it intends to
describe phenomena and requires precise observations, and its research design
makes use of valid and reliable observations (Terre Blanche, Durrheim, &
Painter, 2006:44-45). In a descriptive study, the researcher is required to
possess some prior knowledge of the nature of the problem at hand. However,
before undertaking any action towards a problem, the researcher needs
conclusive evidence which provides answers to the problem. Hence the objective
of descriptive research is to offer an exact image of a marketing environment
(Zikmund & Babin, 2007:42-43), such as:
? Demographic information: In that case the study may help to
describe certain traits of population groups in a given market.
? Behavioural information: Descriptive research may help
describing behaviour patterns of certain population groups.
? Detailed information: Descriptive research offers
information on certain elements by answering questions on: when, how, where,
why, who.
75
For the purpose of this study, a descriptive research was
selected because descriptive research is best used in a survey investigation.
It is ideal for frequencies, average and most statistical calculations and aims
at providing an exact description of people, circumstances or events (Du
Plessis, 2010:118).
4.2.4 Step 4: Conduct secondary research
Secondary data was obtained from various sources such as
journals, books, newspapers and Internet information.
Secondary data was used as part of section 1.7 of Chapter
One, Two and Three. All this data was utilised to supplement the findings of
the research.
4.2.5 Step 5: Select a primary research method
Primary data may be gathered through experimentation,
observations, interviews and written communication. The type of research will
eventually influence the choice of data collection. The method may comprise the
use of self-administered questionnaires, personal and telephonic interviews
that are mainly quantitative by nature (Du Plessis, 2010:118).
4.2.5.1 Data gathering technique
The following section below provides the motives for using
self-administered questionnaires to collect primary data. A research can make
use of different types of surveys such as personal and executive interviews,
mail and telephone surveys. Elements to take into account when choosing a
survey method are (Holder, 2008:72):
· The characteristics of the format in which data is
gathered;
· The quantity and quality of data which can be gathered
using a particular method;
· Control over the sample that differs according to
specific categories of surveys;
· The reliability of data which can be gathered with the
survey type;
· The speed of the research;
· The cost of the selected type of survey.
76
The characteristics of the format in which data is collected
are adapted from Holder (2008:123-125) and applied to the current research. The
reliability of data in the current study is assessed through pre-testing the
questionnaire using five patients who have received medical services at the
military hospital in Libreville, in Gabon. This was performed in order to
determine the time it takes respondents to complete the whole questionnaire,
and to spot and correct any problem in the structure of the questionnaire. The
self-administered questionnaires are handed out directly to the respondents of
the research. This makes the questionnaires easy to administer to all 200
patients and less costly to gather data from respondents compared to other
types of surveys techniques.
4.2.5.2 Self-administered questionnaires
Self-administered questionnaires refer to a survey method
that enables respondents to fill in a questionnaire. Survey questionnaires can
be issued via e-mails, fax, newspapers, Internet or through the place where
service is acquired such as a hotel, restaurant and hospital. They can also be
handed in personally as part of an intercept survey. Depending on the way the
survey is administered, there are a number of sampling framework issues such as
who can or cannot be contacted by fax or Internet, or whether there is a sample
bias. Benefits of a self-administered survey include anonymity of the
respondent in the research that can lead to the acquisition of more honest
answers. The questionnaire can also be completed at the convenience of the
respondent. Since an interviewer is not required, errors or bias due to
interviews is eradicated. The cost of accessing a geographically scattered
sample is cheaper for most types of self-administered surveys than personal or
telephonic surveys. In the majority of self-administered surveys, there is no
influence over who is completing the questionnaire (The Self-Administered
Survey, 2012).
In this study, self-administered questionnaires were handed
to respondents to complete. The respondents in the study had to be 18 years or
older, males and females, who have experienced medical services and stayed over
at the military hospital for at least one night. Data was collected over a
period of three weeks.
77
4.2.5.3 Covering letter
The cover letter informs respondents about the goal of the
research, it should:
· Encourage respondents to be involved in the study;
· Provide the reasons why respondents have been chosen;
and
· Describe the benefits of the research to respondents.
Information provided in the covering letter should influence
the respondent's willingness to be involved in the study (Du Plessis,
2010:120). A covering letter was generated by the researcher. It described the
goal of the research and guaranteed the confidentiality of all respondents'
details and information. A cover letter was issued upon the respondent
request.
4.2.5.4 Questionnaire
The questionnaire included self-administered items initially
developed in English and translated into French, the main language spoken in
the study location. Each translation was verified by professional English and
French translators to ensure that the translations were correct. It is the
major research instrument used for the investigation. A questionnaire
represents an instrument that gathers primary data in survey-based research. It
is composed of well-structured written questions and fixed responses
alternatives directly linked to the purpose of the study (Van Vuuren, 2011:93).
Unlike other forms of surveys, in self-administered questionnaires, researchers
do not actually need to be present during the interview. However, they can
distribute the questionnaires to respondents who are free to read and complete
them at ease (Zikmund & Babin, 2007:143). The benefits of using this
instrument are as follows:
· The researcher can gather all completed questionnaires
within a particular point in time.
· Any question or point that is not clear to respondents
can be explained on the spot.
· The researcher can have the chance to bring in the
research topic and encourage respondents to provide their honest responses
(Munyaradzi, 2010: 215).
· Distributing questionnaires to a large group of people
at the same time appears to be less costly and time consuming than face-to-face
interviews.
78
? However, self-administered questionnaires often require well
through and clarity on the written questions in order for respondents to easily
understand the questionnaires (Zikmund & Babin, 2007:143).
The survey questionnaire is divided into five major sections:
Section A which consists of questions about the respondent's general
demographic information, section B that consists of questions related to the
respondent's perceptions of services, section C that consists of the tangible
aspects of the hospital, section D that relates to the overall perceptions of
services quality, and section E which consists of a list of factors that could
influence the decision to choose the military hospital. The questionnaire
contains 50 questions in total. Section B includes16 statements that measure
the items of service quality based on the reliability, responsiveness,
assurance and empathy dimension. Section B is in the format of a seven-point
Likert-type scale ranging from 1 (strongly disagree) to 7 (strongly agree)
where respondents were given specific limited-alternative responses and asked
to select the one closest to their views. A seven-point Likert-type scale is
best used when the items in the questionnaire are related to each other, or
when the options are in the form of a scale. This type of scale is suitable
when a research aims at getting an overall measurement of a particular topic,
opinion, or experience and also to gather particular data on contributing
factors. Measuring the satisfaction level of a recent service experience is a
common use. (Likert Scale, 2012).
The research questionnaire was adapted from the questionnaire
used by Holder (2008:124) who previously developed and tested items related to
service quality in the hospital industry for their validity and reliability.
4.2.5.5 Questionnaire design
Questionnaires are usually built to capitalise on the
importance and precision of data collected, to capitalise on the involvement of
all respondents in the study, and to facilitate data gathering and their
evaluations. The reasons researchers often use a seven-point Likert-scale are
that they lower the development of response bias among respondents, and they
assess behaviours, beliefs, views and perceptions. Likert-scale responses are
usually not difficult to code and to analyse straight from questionnaires (Du
Plessis, 2010:121).
79
Section A of the questionnaire consists of
eight questions related to the socio-demographic details of the respondents.
This enables the researcher to assess the socio-demographic background of
patients attending the military hospital in Libreville, in Gabon to know if
variables such as age, education, and marital status can influence how patients
rate doctors and nurses on the service quality dimensions in the military
hospital in Libreville, in Gabon. These questions include the following:
1. Gender (Sèxe)
2. Age (Age)
3. Highest educational level (Niveau d'
éducation)
4. Marital status (Statue conjugal)
5. Employment level (Forme d' emploi)
6. Residential area (Lieu de résidence)
7. First time patient? (Est-ce votre première visite
dans cet hôpital?)
8. Were you required to stay over for at least one night?
(Etes-vous obligé de passer au moins une nuit dans cet
hôpital?)
Section B consists of sixteen different
statements on experience of service quality based on the dimensions of service
quality such as reliability, responsiveness, assurance and empathy. The
objective is to compare the views of patients regarding the service delivery by
doctors and nurses at the military hospital. The reliability and the empathy
dimension had five statements each: the responsiveness, the assurance and
tangibility had four statements each. These aspects were adapted from Holder
(2008:124). They are discussed next.
(a) Reliability
Items measuring the influence of reliability on satisfaction
were adapted from Holder (2008:124) who previously developed and tested items
related to the influence of reliability on satisfaction in the hospital
industry. Statements related to reliability include items 1 to 4.
80
The statements read as follows:
The medical doctors/nurses who treated me...:
(Je crois que les médecins /infirmières qui
m'ont traité...)
1. Acted in a way that caused me to trust them (ont
suscité en moi une confiance en eux/elles)
2. Acted in my best interests (ont agi dans mes
intérêts personnels)
3. Had the ability to examine me properly (avaient la
capacité de m'examiné correctement)
4. Were always honest with me (ont été
honnêtes envers moi)
(b) Responsiveness
Items pertaining to the influence of responsiveness on
satisfaction were adapted from Holder (2008:124) who previously developed and
tested items related to the influence of responsiveness on satisfaction in the
hospital industry. Statements related to responsiveness include items 1 to
4.
The statements read as follows:
The medical doctors/nurses who treated me...:
(Je crois que les médecins /infirmières qui
m'ont traité...)
1. Informed me of my state of health during consultation
(m'ont informé sur mon état de santé lors de la
consultation)
2. Communicated the prescription of medications for my treatment
with me in a manner that I could understand (ont utilisé un langage
qui m'a permis de comprendre les prescriptions médicales pour mon
traitement)
3. Always responded to my queries (répondaient
toujours à mes questions)
4. Always listened to what I had to say (faisaient
toujours attention à ce que j'avais à dire)
81
(c) Assurance
Items pertaining to the influence of assurance on satisfaction
were adapted from Holder (2008:124), which include items 1 to 4.
The statements read as follow:
The medical doctors/nurses who treated me...:
(Je crois que les médecins /infirmières qui
m'ont traité...)
1. Showed respect and dignity towards me (m'ont
traité avec beaucoup de respect)
2. Carried out their tasks competently(m'ont traité
avec beaucoup de compétence)
3. Respected the confidentiality of my treatment (ont
respecté la confidentialité de mon traitement)
4. Were well trained and qualified (avaient beaucoup d'
expertise)
(d) Empathy
Items related to the influence of empathy on satisfaction were
adapted from Holder (2008:124), which include items 1 to 4.
The statements read as follow:
The medical doctors/nurses who treated me...:
(Je crois que les médecins /infirmières qui
m'ont traité...)
1. Provided me with individual attention (m'ont
accordé une attention particulière)
2. Were concerned about my well-being (ont montré
beaucoup d'intérêts pour mon bien-être)
3. Understood my specific needs (ont compris mes besoins
personnels
4. Cared about me (ont pris soin de moi)
Section C consists of five different
statements on tangibility and items related to the influence of tangibility on
perceptions of services which were adapted from Holder (2008:124). The
objective is to establish the perception of patients regarding the tangible
aspects of the military hospital in Libreville, Gabon. The statements on
tangibility read as follow:
82
Thinking of the military hospital, I believe.... (Je crois
que...)
1. The furniture in the military hospital such as beds and
chairs was comfortable (le mobilier de l'hôpital tel que les lits et
chaises est confortable)
2. The interior decoration in the military hospital was
aesthetically appealing (J'ai aimé le décor interne de
l'hôpital)
3. The military hospital had a pleasant atmosphere (J'ai
aimé la sensation atmosphérique de l'hôpital)
4. The colour scheme at the military hospital was attractive
(les couleurs de l'hôpital étaient attirantes)
5. The toilet facilities in the military hospital were clean
(Les toilettes étaient propres)
Section D consists of five different statements
on the overall perceptions of the services received from the military hospital.
The objective was to assess how patients perceived the overall services
received from the military hospital.
The statements on overall perceptions of the services received
from the military hospital read as follow:
Thinking of the military hospital, I believe.... (Je crois
que...)
1. The overall quality of the administration service at the
military hospital was excellent (le service administratif de
l'hôpital était excellent)
2. The overall service provided by the military hospital was of
a high standard (le service offert par l'hôpital était en
général de bonne qualité)
3. The overall service I received at the military hospital met
my expectations (les services reçus de l'hôpital se
rapprochent de ce dont j'espérais recevoir)
4. I felt good about coming to this military hospital for my
treatment (je me suis bien senti(e) dans cet hôpital)
5. Overall, the service offering of this hospital was superior
to the one offered by government hospitals (les services offerts dans cet
hôpital étaient meilleurs que ceux offerts par les hôpitaux
publiques)
83
Section E consists of a list of sixteen
factors that could influence the decision to select the military hospital.
These factors were adapted from Doghaither, Abdelrhman, Saeed and Magzoub
(2003:107). The objective was to establish which factor could influence
patients' decision to choose the military hospital in Libreville, Gabon.
The statements read as follows:
1. Availability of modern medical equipment (La
présence d'un équipement médical moderne)
2. Specialised physicians (Les médecins
spécialisés)
3. Quality of nurses (La qualité des
infirmières)
4. Availability of medicines (La disponibilité des
médicaments)
5. Relatives living in the hospital area (Un membre familial
vivant à proximité de l'hôpital)
6. Hospital near residence (La proximité de
l'hôpital du lieu de résidence)
7. Ease of getting to hospital location (L'accès
facile à l'hôpital)
8. Care cost (Le coût des soins hospitalier)
9. Patient's past experience (L'expérience
passée du patient)
10. Competent staff (La compétence du personnel
médical
11. Know people who went to the hospital (Connaissiez-vous
des personnes ayant fréquenté cet hôpital auparavant
?)
12. Good reputation in media (la bonne renommée de
l'hôpital)
13. Hospital cleanliness (l'hôpital est
propre)
14. Employees are friendly towards patient (le personnel est
amical)
15. Hospital is well organised (l'hôpital est bien
organisé)
16. Other? (autres?)
4.2.5.6 Pretesting of the questionnaire
Pretesting a questionnaire is vital to ensure its validity and
reliability. It refers to testing the questionnaire using a small number of
respondents to spot and eliminate any possible error in the survey design
(Malhotra, Hall, Shaw & Oppenheim, 2008:233). Parasuraman, Grewal and
Krishnan (2007:303) stated that pretesting is crucial in a way prospective
respondents may help identifying any problem in the questionnaire. All
84
sections of the questionnaire such as question content,
sequence, wording, form layout and question complexity should actually be
pretested. Additionally, respondents of the small sample must have the same
traits as those included in the current study (Aaker et al., 2007:247). The
purpose of pretesting is to make sure that questions are clear and easy to
understand. Furthermore, pretesting also intends to ensure that questions are
extracting the answers required and that any misinterpreted questions are
eliminated before the questionnaire is distributed to a larger extent
(Munyaradzi, 2010: 222).
The questionnaire was pretested using five patients who had
received medical services at the military hospital in Libreville, Gabon.
Pretesting a questionnaire refers to using it on a trial basis. Pretesting is
important, since it enables knowing that the developed questionnaire is
adequate and will fulfil the purpose of the research at hand. Moreover, the
gathered data will be appropriate and as correct as possible, the target
respondents in the study will participate as fully as possible, and evaluation
of data will run smoothly. In this study, the relevance of pretesting was to
pinpoint flaws in the questionnaire, and to assess the time needed for a
respondent to fill in the entire questionnaire. Pretesting the questionnaire
was also used to examine its face and content validity, and to detect and
correct problem areas. During the pilot study, issues such as the difficulty of
respondents to understand the sentence structures and the difficulty to
understand questions were identified. These issues were addressed by obtaining
suggestions from respondents for revising questions and the structure of
sentences. Once the questionnaire had been pretested, it was then refined for
the data to be gathered (Roberts-Lombard, 2006:41).
4.2.5.7 Reliability and validity of the
questionnaire
Reliability and validity are important elements to evaluate
the trustworthiness of any study. Reliability refers to the extent to which a
scale provides the same outcomes if repeated. To determine the reliability of
the measurement scale in this study, the internal consistency reliability test
was used. It is regarded as an instrument utilised to test the reliability of a
measurement scale or homogeneity among the variables being measured (Malhotra,
2009:315; Churchill & Brown, 2007:269; Saunders, Lewis & Thornhill
(2007:367). The simplest measure of internal consistency is split-half
reliability. The variables on the scale are divided into two halves and the
resulting half scores are compared. High similarities between the halves show
high internal consistency
85
(Parasuraman et al., 2007:270). Additionally, internal
consistency is also used to evaluate the reliability of a summated Likert-scale
where several variables are summated to form a total score. To assess the
reliability of the homogeneity of the measurement scale, the Cronbach's alpha
was used for this research.
Cronbach's alpha is perceived as the average value of the
reliability coefficients one would have for all possible grouping of items when
split into two half-tests. The alpha value is the average of all possible
split-half coefficients that result from different splitting of the items in
the scale. The desired cut-off score for a measurement scale to be reliable is
0.6. Other scores suggest unsatisfactory internal consistency reliability
(Munyaradzi, 2010: 215).
Table 4.1 illustrates the Cronbach alpha values for the
different variables in the study at hand.
Table 4.1: Reliability statistics (Doctors and
Nurses)
|
CONSTRUCTS
|
|
|
Cronbach's Alpha
|
|
DOCTORS
|
NURSES
|
|
Reliability
|
|
|
0.809
|
0.767
|
|
Responsiveness
|
|
|
0.735
|
0.717
|
|
Assurance
|
|
|
0.650
|
0.780
|
|
Empathy
|
|
|
0.734
|
0.666
|
|
Cronbach's Alpha
|
|
|
Tangibility
|
|
0.600
|
|
Table 4.1 illustrates that Cronbach's alpha for all five
constructs is above the lower limit of acceptability, 0.60. This confirms the
reliability of the measurement set for this study. The validity of a scale is
the extent to which it is a true representation of the underlying variable it
is trying to evaluate. Validity is measured using content validity and
construct validity (Parasuraman et al., 2007:269). For the purpose of this
study, content validity was used to assess the accuracy of the measurement
scale.
Content validity can be evaluated by subjective agreement
between experts, that a scale logically seems to accurately measure what it is
intended to measure. Another way to ensure content validity is to use a panel
of people to assess how well an instrument meets the purpose of the study
(Malhotra et al., 2008). In the current study,
86
content validity was determined by people including
statisticians and academics with the expertise for the research at hand. The
questionnaire was evaluated and the necessary modifications were noted both in
terms of the measurement items and the measurement instrument as a whole.
Content validity was evaluated by determining the variables defined and used in
previous literature.
4.2.6 Step 6: Determine the research frame
4.2.6.1 The survey area
The research is conducted at the military hospital situated in
Libreville in Gabon.
4.2.6.2 The study unit
The study is carried out at the military hospital located in
Libreville, Gabon. The research is selected in this city because Libreville is
perceived as the capital, the largest and the most populated city of Gabon.
4.2.6.3 Population
The population refers to the broader group from which sampling
elements are taken and to which results can be summarised. The population
includes all the people which characterize the unit of evaluation. A target
population should be defined in very particular terms. This will make the
selection of respondents from the population for sampling, simpler (Terre
Blanche et al., 2006:133).
Self-administered questionnaires were distributed to all
existing patients of the military hospital in Libreville, Gabon, 18 years or
older, males and females, who had experienced medical services and stayed over
at the military hospital for at least one night. Questionnaires were only given
to them once they have been discharged from hospital.
87
However, individuals who did not experience medical services
at the military hospital were excluded from the study. Figure 4.2 provides a
sum up of the target population, sample units, sample elements and actual
sample size of the study.
Figure 4.2: Target population, sample units, sample
elements and actual sample size

Patients of the military hospital
All patients to the military hospital in Libreville,
Gabon
|
Target population
|
|
|
|
|
|
|
|
|
|
|
|
Sample unit
|
Military hospital in Libreville, Gabon
|
|
Sampling elements
|
|
Patients experiencing services at the military
hospital
|
|
|
|
(Period of March 2013)
|
|
|
|
|
Actual sampling size
|
|
200 patients
|
Source: Researcher's own construct
The sampling technique used to choose a representative sample
for the study was crucial for the research and will be described next.
4.2.6.4 Sampling method
The sampling procedure includes any process using a small
number of constituents from the entire population to draw conclusions related
to the whole population. A sample is an extract of the broader population. The
aim of sampling is to allow researchers to assess some unknown population's
traits. There are two major sampling techniques namely probability and
non-probability sampling. Non-probability sampling is based upon the
researcher's own judgement to choose the sample where he or she chooses what
elements to incorporate. Probability sampling takes place when sampling
constituents are chosen by chance. All units may not necessarily have the same
chance
88
of being chosen, but the probability of choosing each unit can
be specified. Non-probability sampling involves convenience sampling, judgement
sampling, quota sampling and snowball sampling. Probability sampling techniques
encompass simple random, systematic, stratified and cluster sampling (Rahman
& Miazee, 2010:27-28).
In this research, the probability sampling technique was used
to choose respondents in the study, since it constitutes the root for all
survey research (Parasuraman et al., 2007:340).
4.2.6.5 Probability sampling method
This sampling technique was used in this research. Probability
sampling is usually appropriate in survey-based research where one is required
to make interferences from the sample about a population to resolve research
questions. Probability sampling can be divided into four phases:
? Recognise an appropriate sampling framework based on research
objectives;
? Select a proper size of sampling;
? Choose the most suitable sampling method, choose the sample;
and
? Verify that the sample is a good representation of the
population (Holder, 2008:73).
The probability sampling technique was selected for this
research since in this technique, each unit of the population, namely all
patients 18 years or older, males and females, experiencing services at the
military hospital in Libreville, Gabon had a known, non-zero chance of being
incorporated in the sample. Sampling was not conducted at the discretion of the
researcher.
4.2.6.6 Sample technique
In this technique, the probability of each unit being chosen
from the population is known and is often equivalent to all cases. This
indicates that there is a possibility to resolve the research questions by
statistically estimating the population traits from the sample (Parasuraman et
al., 2007:340).
89
There are five major methods which can be utilised throughout
probability sampling. These are (Zikmund & Babin, 2007:273):
? Simple random sampling: In this sampling method, every unit
in the population has a known and same chance of being chosen in the sample.
Each unit is chosen independently. Simple random sampling will comprise of
putting all the units of the population in a container, and extracting the
sample from this.
? Systematic sampling: In this technique, the units of the
population are counted from one to the number of units that constitute the
sample, Prior to completing systematic sampling, the population size should be
divided by the volume of the sample to establish an interval i. The response is
rounded off to the closest integer. If the population is 100 000 units and a
sample of 1 000 is chosen, then one will divide 100 000 per 1 000 which is 100,
to find the interval.
? Stratified sampling: It refers to a two-stage procedure
where the population is primarily divided into strata or subgroups. A
population stratum is a fragment inside that population which has one or more
similar features. These strata must be communally exclusive and jointly
complementary. This implies that every unit must be incorporated into only one
subgroup. In the next stage, units are chosen from every strata or subgroup
through simple random sampling.
? Cluster sampling: With this technique, the population is
divided into communally exclusive and jointly complementary clusters, after
which some clusters are chosen in the sample. Cluster sampling is opposed to
stratified sampling since a variety of clusters must be as similar as possible.
The units of all the clusters will thus have the same traits. The supposition
is thus made that any of the chosen clusters in the sample will correspond to
the clusters which are not chosen in the sample.
? Two and multistage sampling: This method is often utilised
to solve issues related to a geographically dispersed population when
face-to-face contact is required, but will be too costly. Through that method,
a sample is primarily extracted from the population, such as in the
metropolitan regions in Gabon. From it, a second sample will be made, as in
particular residential zone in a metropolitan region and finally, another
sample will be made from that to concentrate only on a particular street in the
residential zone.
Both, stratified sampling and simple random sampling were
conducted in this research. The motive for choosing that sampling method was
that the sampling framework of the research was divided into strata, and the
sampling procedure was conducted
90
independently of each stratum. Stratified samples are
perceived to be very efficient, and they enable investigating the interests of
particular subgroups inside the population. Stratified random sampling provides
better representativeness of the whole population, and also leads to fewer
sampling errors, providing more accuracy in estimation (Du Plessis, 2010:140).
In stratified sampling, strata should be mutually exclusive and jointly
exhaustive in that each population element should be assigned to one and only
stratum and no element should be excluded (Malhotra, 2007:327). The Department
of Internal Medicine of the military hospital in Libreville in Gabon is divided
into four main units, each unit represented an independent stratum.
As there is only one reception in each unit, no further random
selection was required. As all the clinical units were not equal in size and
did not serve an equal number of patients, a proportionate number of patients
who received medical services for at least one night were selected at each unit
(stratum). Self-administered questionnaires were distributed to identify
patients at each unit. Permission to conduct the study was obtained from the
nurse manager of the Department of Internal Medicine of the military hospital
in Libreville in Gabon. The patients interviewed at each clinical unit were
randomly selected. The study made use of a simple random technique where each
population element had not only a known, but an equal chance of being selected
(Munyaradzi, 2010:209). If a patient did not want to be involved in the
research, the next willing patient was selected, and thereafter, the second
patient after each willing one.
4.2.6.7 Sample size
The volume of the sample implies the statistical accuracy of
the findings. The size of the sample is a result of alteration in the
population parameters and the assumption of quality which is needed by the
researcher. In general, bigger samples reduce the likely error in generalising
the population. In other words, larger samples are more representative of the
population and result in more accurate findings. The volume of the sample can
also be decided on the basis of personal judgement and statistical evaluations
(Terre Blanche et al., 2006:236).
In the Gabonese health care industry, though some hospitals
keep records of their patients, this is expected to be a problem for some
medical institutions. The core reason is the durability of the service product
sought by patients from hospitals from time to
91
time. It is difficult to tell when a patient will re-visit and
purchase the service at the hospital. Against this background, the following
formula will be used to estimate the response rate and the actual sample size
needed (Saunders et al., 2007:214):
na = (n x 100) / re
%
With:
na= is the current sample size
needed
n = is the minimum (or
adjusted minimum) sample size
re % = is the estimated
response rate expressed as a percentage
This calculation is based on three major aspects namely the
level of confidence of the accuracy of the estimate, the margin of error which
can be accepted, and the proportion of answers that the researcher expects to
have some particular attribute.
Assuming that the researcher knows the level of confidence and
the margin of error, it will be easier to have an estimation of the proportion
of answers that the researcher expects to receive some particular attribute
(Saunders et al., 2007). In general, researchers use a 95% level of confidence,
which means that if one selects a sample 100 times, at least 95 of these
samples will reflect the true characteristics of the population. The margin of
error relates to the precision of the researcher's estimates of the population.
The standard deviation, also known as error margin usually used in business and
management researches is 5% (Munyaradzi, 2010:211). This means that if 40% of
the researcher's sample lies in a certain category, then the estimate for the
total population within this same category will be 40% plus or minus 5%. For
the purpose of the current study, a 5% margin of error and a 95% confidence
level will be used.
Table 4.2 shows the minimum sample sizes for different sizes
of the population at a 95% confidence level to provide a good decision model
(Saunders et al., 2007:212).
Table 4.2: Minimum sample size estimates
|
Population
|
Five per cent (margin of error)
|
|
100
|
44
|
|
200
|
132
|
|
300
|
168
|
|
400
|
196
|
|
500
|
217
|
Source: Adapted from Munyaradzi (2010:212)
92
Thus, according to this study, a minimum population frame of 100
patients for the military hospital in Libreville, in Gabon was estimated. This
entails that referring to the Table 4.2, the minimum sample which can be
expected is 44 respondents.
According to Saunders et al. (2007:215), a 50% response rate was
suitable for surveys done through questionnaires. Thus, since the current study
uses a questionnaire instrument to gather data, the researcher estimated a 50%
response rate.
According to the formula provided above, the expected sample size
for this research will be:
na = (n x 100) ! re %
na
= 100 x 100 ! 50
na = 200
This entails that the sample size for this study was 200
respondents.
4.2.7 Step 7: Data gathering
Data gathering is the method utilised to gather both primary
and secondary data. Primary data was collected and assessed for the study at
hand (Munyaradzi, 2010: 214). The measuring element for this research was made
through the use of primary data gathered via self-administered survey
questionnaires. This implied that self-administered survey questionnaires were
distributed to all existing patients of the military hospital in Libreville,
Gabon, 18 years or older, males and females, who had experienced services and
stayed over at the military hospital for at least one night.
Secondary data refers to data that has been gathered and
utilised for previous research (Holder, 2008:72). In this study, the researcher
made use of research articles, books, scholar publications, interviews and
Internet sources.
4.2.8 Step 8: Data analysis
Quantitative data represents numerical data which can aid in
providing responses to research questions. This data can vary from simple
calculations such as frequency to more difficult data. To be helpful, the data
should be evaluated and interpreted.
93
Quantitative analysis methods can help in this procedure.
These vary from building simple diagrams which describe the frequency of
occurrence through creating statistical relationships among variables, to more
difficult statistical modelling. It is important to make sure that the data
analysis technique matches the research paradigm and design. Analysing data
starts once data has been gathered. Through the analysis step, various
interrelated processes are undertaken to review and re-organise data. The
stages of data analysis involve editing, coding, processing and statistical
analysis of the data (Terre Blanche et al., 2006:86). To achieve the objective
of this study and to test the hypotheses, SPSS 17.0 for Windows was used to
evaluate data. These different constituents of data analysis are reviewed in
the following sections.
4.2.8.1 Editing of data
Editing is undertaken to ensure that data is prepared for
coding and moved to data storage. It is a procedure for verifying and
correcting the data for omissions, consistency and reliability. Through
editing, questionnaires and the raw data are verified for errors made by either
the researcher or the respondent. The main purpose of editing is to make sure
that the data is correct, consistent with the objective of the questions,
uniformly entered, completed and organised to make coding and tabulation easier
(Du Plessis, 2010:143).
4.2.8.2 Coding of data
Coding is the procedure for giving a code or a number to every
possible answer to a specific question. The aim of coding is to convert the
respondents' responses to survey questions into codes which can be examined and
put into a statistical analysis software package. Precoding can be utilised if
the researcher is aware of what the answer categories will be before gathering
data. In this way, once the questionnaire has been built and the organised
answers have been determined, coding develops into a routine procedure (Du
Plessis, 2010:143).
94
4.2.8.3 Processing and statistical analysis of
data
Various techniques can be used to analyse and interpret
quantitative data. Quantitative data relates to numeric data that the
researcher can use to address the research question. However, a proper
selection of the quantitative technique is a prerequisite to ensure that data
analyses techniques correctly address the research question (Du Plessis,
2010:141). Once data has been gathered, and is ready to be analysed, the
researcher has to perform some basic statistical analyses in order to prepare
data such as data editing, coding and the statistically adjustment of data
(Aaker, 2006:432-434).
? Data editing: The purpose of editing data is to spot any
errors that appeared in the answers. Such errors may have been caused by the
researcher's own error, lack of clarity, contradictions and ineligible
respondents. The researcher may usually return to the study field, address the
missing values or remove unsatisfactory respondents as a way to address these
errors.
? Coding: When all the answers are entered into a computer
file, statistical software will be used to analyse information. However, before
this process occurs, the data has to be verified in terms of any errors which
may have occurred during the process of entering the data. Once the data is
verified, statistical adjustments to the data can be performed.
? Statistical adjustments: Various adjustments to the data are
performed to make them ready for data analysis. Such improvement may be
perceived as weighting, dummy variables, scale transformation and
re-specification (Van Vuuren, 2011:110-111).
The following exact statistical procedures were selected for
their suitability to test the research hypotheses of the study. These
procedures include descriptive statistics such as frequency Tables and
measurement of the mean, as well as measures of dispersion including the
standard deviation. Finally, the paired sample t-test was used to accept or
reject the stated hypotheses. The Statistical Consultation Service of the
University of Johannesburg (STATKON) conducted the analyses. All calculations
were done by means of SPSS.
95
4.3 RALIABILITY OF THE RESULTS
Surveys provide fast, cheap and efficient ways of collecting
information about the population. However, when making use of surveys, the
researcher should reduce the frequent errors found in surveys via defining the
population properly, making sure that the sample corresponds to the population,
and choosing respondents who are available and able to collaborate in the
study. The respondents should also understand the questions and the researcher
should properly understand and fill in the respondents' responses (Du Plessis,
2010:144). The manner in which the researcher dealt with frequent errors is
reviewed next:
4.3.1 Sampling errors
A sample error arises every time the results of the sample
diverge from the values of the population. The phenomenon arises at the time
the investigator shows no concern when the sample is drawn (Du Plessis,
2010:144). In this research, a sample of 200 respondents chosen from all
patients 18 years or older, males and females who had experienced services and
stayed over at the military hospital in Libreville, Gabon for at least one
night, was used to reduce sampling error.
4.3.2 Response errors
This type of errors arises at the time respondents lie or do
not lie intentionally. These errors also happen when the researcher influences
the answers from respondents by highlighting some fact, or when the researcher
makes errors by ticking the incorrect response (Terre Blanche et al.,
2006:152-153). Response errors were reduced by building Likert-type statements
on the questionnaire from related theory and pre-testing the questionnaire to
respondents in the population.
4.3.3 Non-response errors
Non-response errors arise at the time the results of the
respondents in the research differ from what the outcomes would have been if
all the respondents initially chosen, had contributed in the research.
Respondents may not be willing to take part in the research for lack of time or
for lack of interest (Du Plessis, 2010:144).
96
The chosen sample for this research was ideal to ensure
representativeness, and the use of self-administered questionnaires increased
the answer rate as respondents were more willing to take part in the study.
Respondents who refused to cooperate were simply replaced by contacting other
adult patients having experienced medical services at the military hospital in
Libreville, Gabon for at least one night to ensure that a total of 200
respondents were interviewed.
4.4 CONCLUSION
Research methodology was the concern of this chapter. The
chapter dealt with the scope of the survey, the sampling technique, and the way
the survey was organised. The chapter focused on the method of collecting data,
the reasons for choosing the self-administered questionnaire and the value of a
covering letter. Editing, coding, data analysis, the statistical evaluation of
data and the reliability of the results were also addressed in this chapter.
The chapter highlighted the errors that could influence the validity of the
results and the methods that were employed to reduce them. The next chapter
will analyse the research findings and will focus on the answers of the
respondents to the statements in the questionnaire.
97
CHAPTER FIVE: DATA ANALYSIS AND
INTERPRETATION
5.1 INTRODUCTION
Chapter four dealt with the research process and the approach
which was developed for the empirical study. The population, data gathering,
sampling and the questionnaire design were also discussed.
This chapter focuses on analysing and interpreting the results
gathered from the empirical findings. The raw data gathered from the survey
questionnaire must go through preliminary assessment before it can be analysed.
The quality of the results deduced from the statistical techniques and their
subsequent interpretation relies merely on how well the data is prepared and
transformed into a form suitable for analysis (Kumar, Petersen, & Leone,
2007: 437). Data analysis refers to analysing the gathered data and translating
it into results. When data analysis and interpretation are not well conducted,
the research fails to attain what it is intended to measure (Du Plessis,
2010:146).
Descriptive statistics encompassing Tables and more advanced
statistics were utilised to analyse the data which successfully portrays the
relations and trends which were apparent in the study. STATKON helped with the
coding and processing of data which was gathered through the use of
questionnaires.
5.2 MEASUREMENT OF OBJECTIVES AND HYPOTHESES
The primary objective of the study as identified in section
1.5.1 of Chapter 1 is to establish how patients rate doctors and nurses on the
service quality dimensions. Olusoji (2009:7) noted that investigating service
delivery by doctors and nurses and customer satisfaction is vital, as these
variables can influence the loyalty which patients have towards a hospital. He
also argued that a strong correlation exists between services provided by
doctors and nurses, patient loyalty and profitability for hospitals. It is
perceived from this declaration that a good understanding of the services
provided by doctors and nurses that influence patient loyalty, is required to
enhance services and profitability at the military hospital in Libreville in
Gabon. To give effect to the study at
98
hand, the following secondary objectives were deduced (refer to
section 1.5.2 in Chapter 1):
· To determine how patients rate the reliability
of doctors and nurses.
· To establish how patients rate the responsiveness
of doctors and nurses.
· To determine how patients rate the assurance of
doctors and nurses.
· To establish how patients rate the empathy of
doctors and nurses.
· To establish if there is a difference in how patients
rate doctors and nurses on the service quality dimensions.
· To establish the perception of patients regarding the
tangible aspects of a military hospital in Gabon.
The following hypotheses as seen in Chapter 1 section 1.5.3 were
compiled to assist in meeting the secondary objectives of the study. These
hypotheses will be tested for both expected and experience of services provided
by doctors and nurses:
H1: There is no significant difference in how patients rate the
reliability of doctors and nurses.
H2: There is no significant difference in how patients rate the
responsiveness of doctors and nurses.
H3: There is no significant difference in how patients rate the
assurance of doctors and nurses.
H4: There is no significant difference in how patients rate the
empathy of doctors and nurses.
H5: Patients do not have a positive perception of the tangible
aspects of a military hospital in Gabon.
5.3 RESEARCH INSTRUMENT AND RESPONSE
STATISTICS
The study was conducted at the military hospital in Libreville in
Gabon in March 2013 for a period of three weeks. Table 5.1 illustrates a
summary of the number of respondents approached, as well as the response rate
which was obtained.
99
Table 5.1: Respondents' approaches and response
rate
|
Total number of respondents approached to fill in the
self-administered questionnaire
|
200
|
|
Respondent refusal
|
0
|
|
Response rate
|
100%
|
|
Usable questionnaires
|
200
|
|
Usable response rate
|
100%
|
A number of 200 respondents were included in the study. This
was done via using the sampling frame criteria that depicted that only patients
who were at least 18 years of age, males and females, who had experienced
medical services and stayed over at the military hospital for at least one
night, qualified to participate in the study. As indicated Table 5.1, the 200
people who were asked to participate in the study matched the sampling frame.
This gave a response rate of 100%. A total of 200 self-administered
questionnaires were received from the four units of the Department of Internal
Medicine of the military hospital which include; 50 questionnaires received
from the unit that treats malaria and yellow fever, 50 questionnaires received
from the heart diseases unit, 50 questionnaires received from the unit that
monitors patients' health, and 50 questionnaires received from the VIP unit.
5.4 DISCUSSION OF THE RESEARCH FINDINGS
The core of this section is to analyse and interpret the data
that was gathered from respondents who visited the military hospital in
Libreville in Gabon for three weeks during the period of March 2013, and met
the criteria of being part of the study. Results are presented form section A
to E where each section will be presented and discussed. As a result, the
discussion of the findings will be based upon meeting the primary and secondary
research objectives of this current study.
5.4.1 Section A - Demographics
The purpose of this section is to provide the demographic
profile of the respondents in the study (refer to section A of the
questionnaire). Gender, age, education level, marital status, employment level,
residential area, the patient's first visit to the hospital and the
100
question based on knowing if the patient had been required to
stay at the military hospital in Libreville in Gabon, will be discussed under
the demographic section.
Table 5.2 illustrates the frequencies of the demographic
information that was assessed in the study.
Table 5.2: Frequency of selected demographic variables of
the sample
|
Gender
|
|
Variable
|
Frequency
|
Percentage
|
|
Male
|
147
|
74
|
|
Female
|
53
|
26
|
|
Total
|
200
|
100
|
|
Age
|
|
Variable
|
Frequency
|
Percentage
|
|
18 - 28
29 - 38
39 - 49
50 - 60
70 and above
Total
|
34 26 76 40 24 200
|
17 13 38 20 12 100
|
|
Highest education level
|
|
Variable
|
Frequency
|
Percentage
|
|
No formal education Primary education Secondary education
Tertiary education Total
Missing system Total
|
24 6
59
109
198
2
200
|
12 3
30
55
99 1
100
|
|
Marital status
|
|
Variable
|
Frequency
|
Percentage
|
|
Single
Married Divorced Widowed Cohabitant Total
Missing system Total
|
30
127
19
20 1
197
3
200
|
15 64 10 10
1
99 1
100
|
|
Employment level
|
|
Variable
|
Frequency
|
Percentage
|
101
|
Employed full-time Employed part-time Self-employed in formal
sector Self-employed informal sector Unemployed
Student
Pensioner (old age) Total
|
125 14 21 14 2
5
19
200
|
63 7
11
7
1
3
10
100
|
|
Residential area
|
|
Variable
|
Frequency
|
Percentage
|
|
In Libreville
Outside of Libreville Total
|
129
71
200
|
64
36
100
|
From Table 5.2, the results indicated that 147 (74%) of the
respondents were males and 53 (26%) were females. The higher presence of males
in the hospital may be due to the fact since it is a military hospital, males
may have felt more attracted to this hospital compared to females. Over one
third (38%) of the patients were aged between 39 and 49 years old. This large
frequency of patients aged between 39 and 49 years old may be explained by the
fact that there are probably more people in this age category living around the
military hospital area than any other age group. With regard to the level of
education, the majority of respondents (55%) indicated that they have a
tertiary education. This high frequency of tertiary educated people attending
the hospital may be due to the fact that more educated people may have more
knowledge and concerns about their health issues. As a result, this may have
caused them to increasingly visit the hospitals compared to the less educated
patients. With regard to employment level, more than half (63%) of the patients
indicated that they were employed full-time, this could be due to the fact that
the hospital is located in the capital city which has the highest concentration
of economic activities. As a result, most patients attending the hospital and
living in the capital would be likely to be employed. Among the respondents in
the study, almost two-thirds (64%) who visited the hospital, indicated living
in Libreville. This could be explained by the proximity of the hospital to
their place of residence.
102
Main finding 1 (MF1) - There were more male respondents
in the study than females.
Main finding 2 (MF2) - Over one third (38 %) of the
respondents were aged between 39 and 50 years.
Main finding 3 (MF3) - A larger number of respondents in
the study (54.5%) have a tertiary education.
Main finding 4 (MF4) -The majority of respondents (63%)
were employed full-time
Main finding 5 (MF5) - The majority of the respondents in
the study (64%) lived in Libreville.
Table 5.3 Frequency of the number of visits to the
hospital and duration of the visit
|
Frequency of visits
|
Frequency
|
Percentage
|
|
First visit
|
162
|
81.9
|
|
Previous visit(s)
|
37
|
18.6
|
|
Total
|
199
|
100
|
|
Duration of stay
|
Frequency
|
Percentage
|
|
Stayed over for at least one night
|
200
|
100
|
From Table 5.3, the results indicated that 81, 9% of patients
attending the military hospital claimed that it was their first visit to this
hospital. Furthermore, all patients attending the hospital were required to
stay over for at least one night, since the study included only patients
visiting the military hospital and who stayed over for at least one night.
Main finding 6 (MF6) - 81 % of the respondents claimed
that it was their first time to visit the military hospital in Libreville,
Gabon.
Main finding 7 (MF7) - 100 % of the respondents
claimed that they were required to stay at the military hospital in Libreville
in Gabon for at least one night.
103
5.4.2 Section B: Perception of services provided by
doctors and nurses
This section (referring to section B in the questionnaire)
aims at providing the patients' perception of the services provided by doctors
and nurses respectively at the military hospital in Libreville, Gabon. Their
perception of services provided by doctors and nurses was based on four
dimensions of service quality, namely reliability, responsiveness, assurance
and empathy. The purpose of the analysis in this section is to assist in
addressing research objectives 1-4. Tables only reflect response
options where actual responses were recorded.
5.4.2.1 Patient perception of services provided by
doctors and nurses
The following discussion below is based on the statements in
section B of the questionnaire, which aim to provide more clarity on the
opinion of patients regarding the service delivery of doctors and nurses based
on the dimensions reliability, responsiveness, assurance and empathy.
? Reliability (Doctors and Nurses)
The purpose of this discussion is to address secondary objective
1:
«To determine how patients rate the reliability of
doctors and nurses.» ? Doctors' reliability
Table 5.4 indicates the patients' perception of services
provided by doctors with regard to the doctors' reliability.
104
Table 5.4: Patients' perception of doctors'
reliability
|
Doctors
|
Disagree
|
Disagree
somewhat
|
Neutral
|
Agree
somewhat
|
Agree
|
Strongly
agree
|
Total
|
Mean
|
Standard
deviation
|
|
Had the ability to examine me properly
|
|
1
|
0.
|
16.5
|
52.5
|
29.5
|
100
|
6.09
|
0.751
|
|
|
|
5
|
|
|
|
|
|
|
|
Were always honest with me
|
0.5
|
|
1
|
24.5
|
50
|
24
|
100
|
5.96
|
0.778
|
|
Acted in my best interests
|
|
0.5
|
1.
|
22.5
|
60
|
15.5
|
100
|
5.89
|
0.689
|
|
|
|
5
|
|
|
|
|
|
|
|
Acted in a way that caused me to trust
|
0.5
|
1.
|
0.
|
33.5
|
53
|
11.5
|
100
|
5.72
|
0.751
|
|
them
|
|
|
5
|
|
|
|
|
|
|
Table 5.4 illustrates that the majority of respondents, in
terms of answering statements B1 - B4, agreed that they were satisfied with
their interactions with doctors with regard to the doctors' reliability. The
responses have been arranged from most important to least important in terms of
the mean of each response, with reference to the patient's experience of the
services provided by doctors. The mean is defined as the sum of a set of values
divided by their numbers. It is an approximate measure of central location for
metric data (interval and ratio data) only. The process is summarised in the
following formula (Tustin, Ligthelm, Martins & Van Wyk, 2005: 638):
MF8: The mean response for statements B3 (6.09) (Had
the ability to examine me properly) and B4 (5.96) (Were always honest with me)
has the highest means which indicates that patients were most satisfied with
the doctors' ability to examine them properly and to be honest with them in
terms of their medical assessment.
MF9: The mean response for statements B2 (5.89)
(Acted in my best interest) and B1 (5.72) (Acted in a way that caused me to
trust them) rated the lowest mean. Despite the two statements having the lowest
means, patients were still of the opinion that doctors did act in their best
interests and in a manner that caused them to trust them. However, patients
indicated that there was room for
105
improvement in these two aspects of the reliability of
doctors. Such room for improvement could be through improved compassion and
understanding during the diagnoses of the problem.
? Nurses' reliability
Table 5.5 indicates the patients' perception of services provided
by nurses with regard to the nurses' reliability.
Table 5.5: Patients' perception of nurses'
reliability
|
Nurses
|
Agree
somewhat
|
Agree
|
Strongly
agree
|
Total
|
Mean
|
Standard
deviation
|
|
Were always honest with me
|
12
|
64.5
|
23.5
|
100
|
6.12
|
0.586
|
|
Had the ability to examine me properly
|
19
|
66.5
|
14.5
|
100
|
5.96
|
0.578
|
|
Acted in my best interests
|
19
|
69.5
|
11.5
|
100
|
5.93
|
0.549
|
|
Acted in a way that caused me to trust them
|
22
|
71
|
7
|
100
|
5.85
|
0.519
|
Table 5.5 indicates that the majority of respondents, in terms
of answering statements B1 - B4, agreed that they were satisfied with their
interactions with nurses in terms of the reliability of nurses. The responses
have been arranged from most important to least important in terms of the mean
of each response, with reference to the patients' experience of services
provided by nurses.
MF10: The mean response for statements B4 (6.12)
(Were always honest with me), B3 (5.96) (Had the ability to examine me
properly) has the highest means which indicates that patients were most
satisfied with these aspects of the reliability of nurses. Patients indicated
that nurses were honest with them and they had the ability to examine them
properly.
MF11: The mean response for statement B2 (5.93)
(Acted in my best interests) and B1 (5.85) (Acted in a way that caused me to
trust them) rated the lowest mean. Despite the two statements having the lowest
means, patients were still of the opinion that nurses did act in a manner that
caused patients to trust them and delivered a service in their best interests.
However, it was their view that such a service could have been
improved.
106
? Responsiveness (Doctors and Nurses)
The purpose of this discussion is to address secondary objective
2:
«To determine how patients rate the responsiveness of
doctors and nurses.»
? Doctors' responsiveness
Table 5.6 indicates the patients' perception of services provided
by doctors with regard to the doctors' responsiveness.
Table 5.6: Patients' perception of doctors'
responsiveness
|
Doctors
|
Neutral
|
Agree
somewhat
|
Agree
|
Strongly
agree
|
Total
|
Mean
|
Standard
deviation
|
|
Communicated the prescription of medications for my treatment
with me in a manner that I could understand
|
0.
5
|
23
|
38
|
38
|
100
|
6.14
|
0.783
|
|
Always responded to my queries
|
|
18
|
56
|
26
|
100
|
6.08
|
0.660
|
|
Informed me of my state of health during consultation
|
0.5
|
24
|
59
|
16
|
100
|
5.91
|
0.643
|
|
Always listened to what I had to say
|
1
|
30
|
53
|
16
|
100
|
5.84
|
0.690
|
Table 5.6 indicates that the majority of respondents, in terms
of answering statements B5 - B8, agreed that they were satisfied with their
interactions with doctors regarding the responsiveness of the latter towards
patients. The responses have been arranged from most important to least
important in terms of the mean of each response, with reference to the
patients' experience of services provided by doctors.
MF12: The mean response for statements B6 (6.14)
(Communicated the prescription of medications for my treatment with me in a
manner that I could understand) and B7 (6.08) (Always responded to my queries)
has the highest means which indicates that patients were most satisfied with
these aspects of the responsiveness of doctors. The doctors communicated the
prescription of medications for their treatment in a manner they could
understand. In addition, respondents indicated that doctors always responded to
their queries and informed them of their state of health during
consultation.
107
MF13: The mean response for statements B5 (5.89)
(Informed me of my state of health during consultation and) and B8 (5.72)
(Always listened to what I had to say) rated the lowest mean. Despite the two
statements having the lower means, patients were still of the opinion that
doctors do listen to their opinions. However, patients indicated that there was
room for improvement in these two aspects of the responsiveness of doctors.
Such room for improvement could be through improved communication during the
diagnoses of the problem. The feeling was that doctors had to develop more
patience and understanding with patients whilst diagnosing the
patient.
? Nurses' responsiveness
Table 5.7 indicates the patients' perception of services
provided by nurses with regards to the nurses' responsiveness.
Table 5.7: Patients' perception of nurses'
responsiveness
|
Nurses
|
Neutral
|
Agree
somewhat
|
Agree
|
Strongly
agree
|
Total
|
Mean
|
Standard
deviation
|
|
Always listened to what I had to say
|
|
15.
|
60
|
24.
|
100
|
6.0
|
0.628
|
|
|
5
|
|
5
|
|
9
|
|
Communicated the prescription of medications for my
|
|
13
|
64.
|
22.
|
100
|
6.1
|
0.590
|
treatment with me in a manner that I could understand
|
|
|
5
|
5
|
|
|
|
Always responded to my queries
|
|
16
|
68.
|
15.
|
100
|
6
|
0.563
|
|
|
|
5
|
5
|
|
|
|
Informed me of my state of health during consultation
|
1
|
16.
|
70.
|
12
|
100
|
5.9
|
0.568
|
|
|
|
5
|
5
|
|
|
4
|
|
Table 5.7 indicates that the majority of respondents, in terms
of answering statements B5 - B8, agreed that they were satisfied with their
interactions with nurses in terms of their responsiveness. The responses have
been arranged from most important to least important in terms of the mean of
each response, with reference to the patients' experience of services provided
by nurses.
MF14: The mean response for statements B8 (6.09)
(Always listened to what I had to say), B6 (6.1) (Communicated the prescription
of medications for my treatment with me in a manner that I could understand)
has the highest means which
108
indicates that patients were most satisfied with these
aspects regarding the responsiveness of nurses. Respondents indicated that
nurses always listened to what patients had to say and communicated the
prescription of medications for their treatment in a manner that they could
understand.
MF15: The mean response for statements B7 (6.0)
(Always responded to my queries) and B5 (5.94) (Informed me of my state of
health during consultation) was the lowest. Despite the two statements having
the lowest means, patients were still of the opinion that nurses informed them
of their state of health during consultation and always responded to their
queries. However, this aspect of responsiveness could have been
improved.
? Assurance (Doctors and Nurses)
The purpose of this discussion is to address secondary objective
3:
«To determine how patients rate the assurance of doctors
and nurses.» ? Doctors' assurance
Table 5.8 indicates the patients' perception of services
provided by doctors with regards to the doctors' assurance.
Table 5.8: Patients' perception of doctors'
assurance
|
Doctors
|
Disagree
somewhat
|
Neutral
|
Agree
somewhat
|
Agree
|
Strongly
agree
|
Total
|
Mean
|
Standard
deviation
|
|
Were well trained and qualified
|
0.5
|
5.5
|
12.5
|
70
|
11.5
|
100
|
5.87
|
0.699
|
|
Showed respect and dignity towards me
|
|
1.5
|
19.5
|
70
|
8.5
|
100
|
5.86
|
0.567
|
|
Carried out their tasks competently
|
|
2
|
20.5
|
69
|
8.5
|
100
|
5.84
|
0.588
|
|
Respected the confidentiality of my
treatment
|
|
4.5
|
30
|
49
|
16.5
|
100
|
5.78
|
0.773
|
Table 5.8 indicates that the majority of respondents, in terms
of answering statements B9 - B12, agreed that they were satisfied with their
interactions with doctors with regard to the assurance that doctors provided to
patients. The responses have been arranged
109
from most important to least important in terms of the mean of
each response, with reference to the patients' experience of services provided
by doctors.
MF16: The mean response for statements B12 (5.87)
(Were well trained and qualified), B9 (5.86) (Showed respect and dignity
towards me) and B10 (5.84) (Carried out tasks competently) has the highest
means which indicates that patients were most satisfied with these aspects of
the assurance of doctors. The doctors were well trained and qualified; they
showed respect and dignity towards patients, and carried out their tasks
competently.
MF17: The mean response for statement B11 (5.78)
(Respected the confidentiality of my treatment) rated the lowest mean. Patients
were of the opinion that doctors respected the confidentiality of their
treatment. However, this could have been improved.
MF18: Patients were of the opinion that doctors were
successful in creating assurance, however they were less successful in
achieving assurance than achieving reliability and responsiveness as recorded
by the lower mean scores in the assurance dimension compared to the mean scores
in the reliability and responsiveness dimensions of doctors'
services.
? Nurses' assurance
Table 5.9 indicates the patients' perception of services
provided by nurses with regard to the nurses' assurance.
Table 5.9: Patients' perception of nurses'
assurance
|
Nurses
|
Neutral
|
Agree
somewhat
|
Agree
|
Strongly
agree
|
Total
|
Mean
|
Standard
deviation
|
|
Respected the confidentiality of my treatment
|
1.5
|
10.6
|
33.3
|
54.5
|
100
|
6.41
|
0.74
|
|
Carried out their tasks competently
|
1.5
|
10.6
|
39.9
|
48
|
100
|
6.34
|
0.729
|
|
Were well trained and qualified
|
2
|
8.1
|
49
|
40.9
|
100
|
6.29
|
0.7
|
|
Showed respect and dignity towards me
|
|
12.1
|
58.6
|
29.3
|
100
|
6.17
|
0.622
|
110
Table 5.9 indicates that the majority of respondents, in terms
of answering statements B9 - B12, agreed that they were satisfied with their
interactions with nurses in terms of their assurance. The responses have been
arranged from most important to least important in terms of the mean of each
response, with reference to the patients' experience of services provided by
nurses.
MF19: The mean response for statements B11 (6.41)
(Respected the confidentiality of my treatment), B10 (6.34) (Carried out their
tasks competently) and B12 (6.29) (Were well trained) has the highest means
which indicates that patients were most satisfied with these aspects regarding
the assurance of nurses. Respondents indicated that nurses respected the
confidentiality of their treatment, they carried out their tasks competently,
and were well trained and qualified
MF20: The mean response for statement B9 (6.17)
(Showed respect and dignity towards me) was the lowest in terms of the
assurance perception of nurses by patients. Despite the statement having the
lowest mean, patients were of the opinion that nurses do show respect and
dignity towards them. However, this aspect of assurance could have been
improved.
? Empathy (Doctors and Nurses)
The purpose of this discussion is to address secondary objective
4:
«To determine how patients rate the empathy of doctors
and nurses.» ? Doctors' empathy
Table 5.10 indicates the patients' perception of services
provided by doctors with regards to the doctors' empathy.
111
Table 5.10: Patients' perception of doctors'
empathy
|
Doctors
|
Neutral
|
Agree
somewhat
|
Agree
|
Strongly
agree
|
Total
|
Mean
|
Standard
deviation
|
|
Were concerned about my well- being
|
2
|
15.5
|
57.5
|
25
|
100
|
6.06
|
0.696
|
|
Cared about me
|
2
|
12
|
74
|
12
|
100
|
5.96
|
0.566
|
|
Provided me with individual
attention
|
1
|
17
|
72.5
|
9.5
|
100
|
5.91
|
0.545
|
|
Understood my specific needs
|
2
|
25
|
53.5
|
19
|
100
|
5.90
|
0.719
|
Table 5.10 indicates that the majority of respondents, in
terms of answering statements B13 - B16, agreed that they were satisfied with
their interactions with doctors in terms of the empathy that doctors had
towards them. The responses have been arranged from most important to least
important in terms of the mean of each response, with reference to the
patients' experience of services provided by doctors.
MF21: The mean response for statements B14 (6.06)
(Were concerned about my well-being), B16 (5.96) (Cared about me) has the
highest means which indicates that patients were most satisfied with these
aspects of the empathy of doctors. Patients responded that doctors showed real
concern for their well-being, and that they cared about them as
individuals.
MF22: The mean response for statement B13 (5.91)
(Provided me with individual attention) and B15 (5.90) (Understood my specific
needs) rated the lowest means. Despite the two statements having the lowest
means, patients were of the opinion that doctors did provide them with
individual attention and understood their specific needs. However, they
indicated that there was room for improvement.
MF23: Considering the mean results discussed,
patients were of the opinion that doctors were successful in achieving
reliability, responsiveness, assurance and empathy.
? Nurses' empathy
Table 5.11 indicates the patients' perception of services
provided by nurses with regard to the nurses' empathy.
112
Table 5.11: Patients' perception of nurses'
empathy
|
Nurses
|
Neutral
|
Agree
somewhat
|
Agree
|
Strongly agree
|
Total
|
Mean
|
Standard deviation
|
|
Were concerned about my well-being
|
|
2
|
18
|
80
|
100
|
6.78
|
0.461
|
|
Understood my specific needs
|
0.5
|
2
|
24.5
|
73
|
100
|
6.7
|
0.530
|
|
Cared about me
|
|
2
|
28.5
|
69.5
|
100
|
6.68
|
0.511
|
|
Provided me with individual attention
|
|
4
|
34.5
|
61.5
|
100
|
6.58
|
0.571
|
Table 5.11 indicates that the majority of respondents, in
terms of answering statements B13 - B16, agreed that they were satisfied with
their interactions with nurses in terms of their empathy. The responses have
been arranged from most important to least important in terms of the mean of
each response, with reference to the patients' experience of services provided
by nurses.
MF24: The mean response for statements B11 (6.78)
(Were concerned about my well-being), B15 (6.70) (Understood my specific needs)
and B16 (6.68) (Cared about me) has the highest means which indicates that
patients were most satisfied with these aspects regarding the empathy of
nurses. Respondents indicated that nurses were concerned about their
well-being; they understood their specific needs, and cared about
them.
MF25: The mean response for statement B13 (6.58)
(Provided me with individual attention) was the lowest in terms of the empathy
perception of nurses by patients. Despite the statement having the lowest mean,
patients were of the opinion that nurses provided them with individual
attention, but that this aspect of empathy could have been
improved.
5.4.2.2 Comparing patient perception of services
delivered by doctors and nurses
The following discussion is based on the statements in section
B of the questionnaire. The aim of the discussion is to provide more clarity on
the differences of opinion of patients regarding the service delivery by
doctors and nurses based on the four
113
dimensions of service quality (reliability, responsiveness,
assurance and empathy). It will furthermore aim to address objective 5,
namely:
«To establish if there is a difference in how patients
rate doctors and nurses on the
service quality dimensions»
The paired sample t-test was used to establish whether
significant differences exist in how patients rate the service delivery of
doctors and nurses based on the four dimensions of service quality.
? Reliability
Reliability statistics for doctors and nurses compared by
means
Table 5.12: Overall mean scores, standard deviations and
p-value for the reliability of doctors and nurses
|
Category
|
Overall Mean
|
Standard
Deviation
|
Significance
(2-tailed)
|
|
Doctors
|
5.912
|
.5924
|
.238
|
|
Nurses
|
5.961
|
.4283
|
MF26: Patients were of the opinion that nurses were
overall more successful in achieving reliability compared to doctors as
recorded by the higher mean scores obtained for the reliability statements
relating to nurses (refer to Table 5.12). The research at hand relies on a 95%
level of confidence, therefore a p-value equal or less than 0.05 implies that
the results are not subject to change according to the paired sample t-test.
Hence a value smaller than 0.05 indicates a significant difference between how
patients perceive the reliability of doctors and nurses. Therefore, considering
a p-value of 0.238, patients do not perceive the reliability of doctors and
nurses significantly differently.
? Responsiveness
Responsiveness statistics for doctors and nurses compared
by means
114
Table 5.13: Overall mean scores, standard deviations
and p-value for the responsiveness of doctors and nurses
|
Category
|
Overall Mean
|
Standard
Deviation
|
Significance
(2-tailed)
|
|
Doctors
|
5.992
|
.5196
|
.350
|
|
Nurses
|
6.028
|
.4320
|
MF27: Patients were of the opinion that nurses were
overall more successful in achieving responsiveness compared to doctors as
recorded by the higher mean scores obtained for the responsiveness statements
relating to nurses (refer to Tables 5.13). The research at hand relies on a 95%
level of confidence, therefore a p-value equal or less than 0.05 implies that
the results are not subject to change according to the paired sample t-test.
Hence, a value smaller than 0.05 indicates a significant difference between how
patients perceive the responsiveness of doctors and nurses. Therefore,
considering a p-value of 0.350, patients do not perceive the responsiveness of
doctors and nurses as being significantly different.
? Assurance
Assurance statistics for doctors and nurses compared by
means
Table 5.14: Overall mean scores, standard deviations
and p-values for the assurance of doctors and nurses
Category
|
Overall Mean
|
Standard
Deviation
|
Significance
(2-tailed)
|
Doctors
|
5.835
|
.4624
|
.000
|
Nurses
|
6.303
|
.5429
|
|
MF28: Patients were of the opinion that nurses were
overall more successful in achieving assurance compared to doctors as recorded
by the higher mean scores obtained for the assurance statements relating to
nurses (refer to Table 5.14). The research at hand relies on a 95% level of
confidence, therefore a p-value equal or less than 0.05 implies that the
results are not subject to change according to the
115
paired sample t-test. Hence, a value smaller than 0.05
indicates a significant difference between how patients perceive the assurance
of doctors and nurses. Therefore, considering a p-value of 0.000, patients do
perceive the assurance provided by doctors and nurses as significantly
different.
? Empathy
Empathy statistics for doctors and nurses compared by
means
Table 5.15: Overall mean scores, standard deviations
and p-values for the empathy of doctors and nurses
|
Category
|
Overall Mean
|
Standard
Deviation
|
Significance
(2-tailed)
|
|
Doctors
|
5.953
|
.4742
|
.000
|
|
Nurses
|
6.303
|
.5429
|
MF29: Patients were of the opinion that nurses were
overall more successful in achieving empathy compared to doctors as recorded by
the higher mean scores obtained for the assurance statements relating to nurses
(refer to Tables 5.15). The research at hand relies on a 95% level of
confidence, therefore a p-value equal or less than 0.05 implies that the
results are not subject to change according to the paired sample t-test. Hence,
a value smaller than 0.05 indicates a significant difference between how
patients perceive the empathy of doctors and nurses. Therefore, considering a
p-value of 0.000, patients do perceive the empathy provided by doctors and
nurses as significantly different.
5.4.3 Section C: Perceptions of patients towards the
tangibility dimension of the hospital
This section (referring to section C in the questionnaire)aims
at providing the patients' perception regarding the tangible aspects of a
military hospital in Gabon. Five statements were used to measure patient
opinion on the tangibility dimension of service quality. The results of this
section will assist in addressing research objective 6, namely:
116
«To establish the perception of patients regarding the
tangible aspects of a military hospital in Gabon»
Please note that Table 5.16 only reflect response options
where actual responses were recorded.
The results are discussed in Table 5.16.
Table 5.16: Tangible aspects
|
Tangibility
|
Neutral
|
Agree
somewhat
|
Agree
|
Strongly
agree
|
Total
|
Mean
|
Standard
deviation
|
|
The toilet facilities in the hospital were clean
|
0.5
|
2
|
69.5
|
28
|
100
|
6.25
|
.509
|
|
The colour scheme at the hospital was attractive
|
0.5
|
3
|
71
|
25.5
|
100
|
6.22
|
.510
|
|
The hospital had a pleasant atmosphere
|
0.5
|
12.5
|
59.5
|
27.5
|
100
|
6.14
|
.634
|
|
The interior decoration at the hospital was
aesthetically appealing
|
0.5
|
18
|
60
|
21
|
100
|
6.01
|
.675
|
|
The furniture at the hospital such as beds and chairs was
comfortable
|
11.5
|
7.5
|
65
|
16
|
100
|
5.86
|
.823
|
Table 5.16 indicates that the majority of respondents agreed
that they were satisfied with the tangible aspects of the military hospital.
The responses have been arranged from most important to least important in
terms of the mean of each response, with reference to the patients' perceptions
of the tangible aspects.
MF 30: The mean response for statements C1 (6.25),
(6.22), C3 (6.14) has the highest means which indicates that patients were most
satisfied with these aspects of the tangible aspects. Respondents indicated
that the toilet facilities in the hospital were clean; the colour scheme at the
hospital was attractive, and the military hospital had a pleasant
atmosphere
117
MF 31: The mean response for statements C4 (6.01) and
C5 (5.86) rated the lowest mean. Despite the two statements having the lowest
means, patients were still of the opinion that the interior decoration at the
hospital was aesthetically appealing and the furniture at the hospital such as
beds and chairs was comfortable. However, patients indicated that there was
room for improvement in these two aspects of the tangible aspects. Such room
for improvement could be through changing the furniture and the interior
decoration at the hospital on a regular basis.
Table 5.17: Overall mean scores and standard
deviations for the tangibility dimension of service quality as rated by the
respondents
|
Category
|
Overall Mean
|
Standard
Deviation
|
|
Tangibility
|
6.0538
|
.49929
|
MF32: Patients were overall satisfied with the
tangible aspects of the hospital in Libreville, Gabon as recorded by the high
mean scores obtained for the tangibility statements relating to the hospital
(refer to Table 5.17).
5.4.4 Section D: Overall perception of
services
This section (referring to section D in the questionnaire)aims
at providing the patients' overall perception of services provided at a
military hospital in Gabon. Five statements were used to measure patients'
overall perception of services. The results are discussed in Table 5.18.
Tables only reflect response options where actual responses were
recorded.
Table 5.18: Overall perception of services
|
Overall perception of services
|
Neutral
|
Agree
Somewhat
|
Agree
|
Strongly
agree
|
Total
|
Mean
|
Standard
deviation
|
|
Overall, the service offering of this military hospital was
superior to the one offered by governments hospitals
|
|
1.5
|
78.5
|
20
|
100
|
6.19
|
0.426
|
118
|
The overall service provided by the military hospital was of a
high standard
|
|
18
|
46.5
|
35
|
100
|
6.18
|
0.712
|
|
I felt good about coming to this military hospital for my
treatment
|
|
15
|
57
|
28
|
100
|
6.13
|
0.644
|
|
The overall quality of the administration service at the
military hospital was excellent
|
0.5
|
17
|
62
|
20.5
|
100
|
6.03
|
0.630
|
|
The overall service I received at the military hospital met my
expectations
|
10.5
|
7.5
|
54.0
|
28
|
100
|
6
|
0.883
|
Table 5.18 indicates that the majority of respondents agreed
that they were satisfied with the overall services provided at the military
hospital. The responses have been arranged from most important to least
important in terms of the mean of each response, with reference to the
patients' overall perceptions of services provided at the military hospital.
MF 33: The mean response for statements D5 (6.19), D2
(6.18), D4 (6.13) has the highest means which indicates that patients were most
satisfied with these aspects of the overall perception of services provided.
Respondents indicated that overall, the service offering of this military
hospital was superior to that offered by government hospitals. The overall
service provided by the military hospital was of a high standard and they felt
good about coming to this military hospital for their treatment.
MF 34: The mean response for statements D3 (6.03) and
D1 (6) rated the lowest mean. Despite the two statements having the lowest
means, patients were still of the opinion that the overall quality of the
administration service at the military hospital was excellent and the overall
service they received at the military hospital met their expectations. However,
patients indicated that there was room for improvement in these two aspects of
the overall perception of services provided. Such room for improvement could be
through improved administration, and doctors' and nurses' services
delivery.
119
Table 5.19: Overall means score and standard deviation
for the overall perception of service delivery as rated by the
respondents
|
Category
|
Overall Mean
|
Standard
Deviation
|
|
Overall perception of service delivery
|
6.281
|
2.506
|
MF32: Patients were overall satisfied with the
tangible aspects of the hospital in Libreville, Gabon as recorded by the high
mean score obtained for the tangibility statements relating to the hospital
(refer to Table 5.19).
5.4.5 Section E: Factors that could influence the choice
for the military hospital
This section (referring to section E in the questionnaire)
aims at providing a list of factors that could influence patients' choice for
the military hospital in Gabon. Sixteen statements were used to determine the
influential factors for selecting the military hospital. The results are
discussed in Table 5.20.
Table 5.20: Influential factors
|
Factors
|
Not at all
important
|
Low
importance
|
Neutral
|
Moderately
important
|
Extremely
important
|
Total
|
Mean
|
Standard
deviation
|
|
Availability of medicines
|
|
0.5
|
0.5
|
11.5
|
87.5
|
100
|
4.86
|
0.402
|
|
Specialised physicians
|
|
|
1.5
|
12
|
86.5
|
100
|
4.85
|
0.398
|
|
Availability of modern medical equipment
|
|
|
1.5
|
13.5
|
85
|
100
|
4.84
|
0.411
|
|
Hospital cleanliness
|
|
0.5
|
2
|
12
|
85.5
|
100
|
4.83
|
0.464
|
|
Employees are friendly towards patients
|
|
|
|
18
|
82
|
100
|
4.82
|
0.385
|
|
Hospital is well organised
|
|
|
1.5
|
21.5
|
77
|
100
|
4.76
|
0.465
|
|
Quality of nurses
|
|
|
1
|
22
|
77
|
100
|
4.76
|
0.451
|
|
Other
|
|
|
|
25
|
75
|
100
|
4.75
|
0.500
|
|
Ease of getting to hospital location
|
|
0.5
|
2.5
|
18.5
|
78.5
|
100
|
4.75
|
0.519
|
|
Competent staff
|
|
11.5
|
2.5
|
14
|
72
|
100
|
4.47
|
0.997
|
|
Good reputation in media
|
2
|
7.5
|
13.5
|
23
|
54
|
100
|
4.2
|
1.060
|
|
Care cost
|
|
6.5
|
13
|
37.5
|
43
|
100
|
4.17
|
0.892
|
|
Patients' past experience
|
1.5
|
10.1
|
22.2
|
35.9
|
30.3
|
100
|
3.83
|
1.021
|
|
Hospital near residence
|
1
|
10.5
|
23.5
|
37.5
|
27.5
|
100
|
3.8
|
0.992
|
|
Know people who went to the hospital
|
1.5
|
11.5
|
30.5
|
29
|
27.5
|
100
|
3.7
|
1.043
|
|
Relatives living in the hospital area
|
2.5
|
18.5
|
7
|
56.5
|
15.5
|
100
|
3.64
|
1.032
|
120
121
Table 5.20 indicates that the majority of respondents agreed
that their choice for the military hospital was influenced by a number of
factors. The responses have been arranged from most important to least
important in terms of mean of each response, with reference to a list of
factors that could influence patients' choice for the military hospital in
Gabon.
MF 35: The mean response for statements E1 (4.86), E2
(4.85), E3 (4.84), E4 (4.83), E5 (4.82), E6 (4.76), E7 (4.76), E8 (4.75) and E9
(4.75) has the highest means which indicates that these factors, E1 (4.86), E2
(4.85), E3 (4.84), E4 (4.83), E5 (4.82), E6 (4.76), E7 (4.76), E8 (4.75) and E9
(4.75) had more influence in patients' choice for the military
hospital.
MF 36: The mean response for statements E10 (4.47),
E11 (4.2) and E12 (4.17) rated the lowest mean which indicates that these
factors, E10 (4.47), E11 (4.2) and E12 (4.17) had less influence on patients
choice for the military hospital.
5.5 ACCEPTANCE OR REJECTION OF HYPOHESES
The hypotheses developed in Chapter 1 will now be dealt with
(refer to section 1.5.3).
H01: There is no significant difference in how patients rate
the reliability of doctors and nurses.
HA1: There is a significant difference in how patients rate
the reliability of doctors and nurses.
H02: There is no significant difference in how patients rate
the responsiveness of doctors and nurses.
HA2: There is a significant difference in how patients rate
the responsiveness of doctors and nurses
H03: There is no significant difference in how patients rate
the assurance of doctors and nurses.
HA3: There is a significant difference in how patients rate
the assurance of doctors and nurses.
122
H04: There is no significant difference in how patients rate
the empathy of doctors and nurses.
HA4: There is a significant difference in how patients rate
the empathy of doctors and nurses.
H05: Patients do not have a positive perception of the
tangible aspects of a military hospital in Libreville, Gabon.
HA5: Patients do have a positive perception of the tangible
aspects of a military hospital in Libreville, Gabon.
The following hypotheses: H01, which states that there is no
significant difference in how patients rate the reliability of doctors and
nurses, H02, which states that there is no significant difference in how
patients rate the responsiveness of doctors and nurses, and the following
alternative hypotheses HA3, which states that there is a significant difference
in how patients rate the assurance of doctors and nurses, HA4, which states
that there is a significant difference in how patients rate the empathy of
doctors and nurses, HA5, which states that patients do have a positive
perception of the tangible aspects of a military hospital in Libreville, Gabon
are therefore accepted.
The following alternative hypothesis: HA1, which states that
there is a significant difference in how patients rate the reliability of
doctors and nurses, HA2, which states that there is a significant difference in
how patients rate the responsiveness of doctors and nurses, and the following
null hypotheses H03, which states that there is not a significant difference in
how patients rate the assurance of doctors and nurses, H04, which states that
there is not a significant difference in how patients rate the empathy of
doctors and nurses, and the H05, which states that patients do not have a
positive perception of the tangible aspects of the military hospital in
Libreville, Gabon are therefore rejected.
5.6 MEASUREMENT OF THE OBJECTIVES
The purpose of this research was to assess the service quality
of doctors and nurses at the military hospital in Libreville (refer to section
1.4). The objectives of the study were
123
assessed empirically via a survey questionnaire. Section A of
the questionnaire collected the demographic details of respondents. Section B
gathered information on patients' experience of services of doctors and nurses
based on the four dimensions of service quality namely reliability,
responsiveness, assurance and empathy. Section C gathered information on
patients' perceptions of the tangibility aspects and overall service quality.
Section D tested the overall perception of patients regarding the service
delivery at the military hospital in Libreville, Gabon. Section E gathered
information on factors that could influence patients' decision to select the
military hospital in Libreville, Gabon. The objectives of this study were
assessed by concentrating on the following aspects:
· A comprehensive literature review was provided on the
nature of the service sector, service quality and patient satisfaction, the
elements of service quality, and how they influence patient satisfaction.
· The empirical study tested the hypothesis that there
is no difference in how patients rate the reliability of doctors and nurses.
· The empirical study tested the hypothesis that there
is no difference in how patients rate the responsiveness of doctors and
nurses.
· The empirical study tested the hypothesis that there
is no difference in how patients rate the assurance of doctors and nurses.
· The empirical study tested the hypothesis that there
is no difference in how patients rate the empathy of doctors and nurses.
· The empirical study tested the hypothesis that
patients do not have a positive perception of the tangible aspects of a
military hospital in Gabon.
5.7 CONCLUSION
The objective of this research was to establish if there is a
difference in how patients rate doctors and nurses on the service quality
dimensions. Chapter five covered the analysis and interpretation of the results
of the data gathered from the survey questionnaires that were completed by the
respondents in the study. The major findings in the research were that there is
no significant difference in how patients rate the reliability and
responsiveness of doctors and nurses, there is a significant difference in how
patients rate the assurance and empathy of doctors and nurses and patients do
have a positive perception of the tangible aspects of the military hospital.
Therefore,
124
H01, H02, HA3, HA4 and HA5 were accepted. The next chapter
will focus on the conclusions related to this research.
125
CHAPTER SIX: CONCLUSIONS, IMPLICATIONS AND
RECOMMENDATIONS
6.1 INTRODUCTION
Chapter five dealt with the research results which were
gathered from the empirical exploration, as well as the major findings. The
goal of Chapter Six is to make a number of conclusions, implications and
recommendations from Chapter Five and the entire study.
The primary objective of this research as seen in Chapter 1
(refer to 1.5.1), was to establish how patients rate doctors and nurses on the
service quality dimensions at a military hospital in Libreville, Gabon.
Secondary objectives were also made in Chapter 1 (refer to
1.5.2) in order to complement the primary objective. The secondary objectives
will again be introduced in section 6.2 and will deal with the relevant major
findings from this research. Each secondary objective will be discussed
followed by a discussion on the implications and recommendations. Chapter Six
will end with a discussion on the limitations and recommendations for more
research to be undertaken.
6.2 MAIN CONCLUSIONS, IMPLICATIONS AND RECOMMENDATIONS OF
THE STUDY
In this research, one major aspect was investigated which was
to establish how patients rate doctors and nurses on the service quality
dimensions. This aspect constituted the core within in which the secondary
objectives as illustrated in Chapter 1.5.2 were established. This chapter will
be based on a discussion of the main conclusions, implications and
recommendations of the findings of each secondary objective.
126
6.2.1 Perceptions of patients regarding the four service
quality dimensions investigated in this study
The secondary objectives of this study related to perceptions of
patients regarding the four service quality dimensions, were determined as
follows:
? To determine how patients rate the reliability of
doctors and nurses. ? To establish how patients rate the responsiveness
of doctors and nurses. ? To determine how patients rate the assurance
of doctors and nurses. ? To establish how patients rate the empathy
of doctors and nurses.
The following hypotheses resulted from the above secondary
objectives:
H1: There is no significant difference in how patients rate the
reliability of doctors and nurses.
H2: There is no significant difference in how patients rate the
responsiveness of doctors and nurses.
H3: There is no significant difference in how patients rate the
assurance of doctors and nurses.
H4: There is no significant difference in how patients rate the
empathy of doctors and nurses.
H5: Patients do not have a positive perception of the tangible
aspects of a military hospital in Gabon.
The major findings in terms of patients' perceptions regarding
the reliability, responsiveness, assurance and empathy of doctors and nurses
were as follows:
- There is no significant difference in how patients rate the
reliability of doctors and nurses.
- There is no significant difference in how patients rate the
responsiveness of doctors and nurses.
- There is a significant difference in how patients rate the
assurance of doctors and
127
nurses.
- There is a significant difference in how patients rate the
empathy of doctors and nurses.
The major findings derived from the empirical research phase
in terms of patients perceptions of service delivery of doctors relating to the
four dimensions of service quality are indicated next:
In terms of reliability, it is clear from the results obtained
that the majority of respondents were satisfied with their interactions with
doctors with regard to the doctors' reliability. Patients indicated that they
were most satisfied with the doctors' ability to examine them properly and to
be honest with them in terms of their medical assessment. Patients were however
of the opinion that there was room for improvement in the way doctors acted in
their best interests, and in the way that caused them to trust them. Such room
for improvement could be through improved compassion and understanding during
the diagnoses of the problem. Such an improvement could enhance their
satisfaction level with the reliability of doctors.
In terms of responsiveness, the results indicated that the
majority of respondents were satisfied with their experience of doctors'
responsiveness. Respondents indicated that they were most satisfied with the
way doctors communicated the prescription of medications for their treatment in
a manner they could understand and the fact that they always responded to their
queries. Patients were however of the opinion that doctors could listen to them
more, and inform them of their state of health during consultation. Such room
for improvement could be through improved communication during the diagnoses of
the problem. The feeling was that doctors had to develop more patience and
understanding with patients whilst diagnosing the patient.
In terms of assurance, it was evident that the majority of
respondents were satisfied with the dealings they had had with doctors with
regard to the doctors' assurance. Respondents indicated that they were most
satisfied with the doctors' trainings and qualifications, the way they carried
out tasks competently and the respect and dignity they as patients received
from doctors. Respondents were however of the opinion that doctors could show
more respect in terms of the confidentiality of treatment. Such an improvement
could be through improved work ethic in the hospital, where patients' records
and cases should never be discussed with anyone without the patients'
128
permission. Patients also indicated that doctors were less
successful in achieving assurance than achieving reliability and responsiveness
as recorded by the lower mean scores in the assurance dimension, compared to
the mean scores in the reliability and responsiveness dimension of doctors'
services.
In terms of empathy, the results indicated that the majority
of patients were satisfied with the dealings they had had with doctors with
regard to the doctors' empathy. Patients indicated that that they were most
satisfied with the doctors' concerns about their well-being and the way they
cared for them. Patients were however of the opinion that doctors could
understand their specific needs better and provide them with more individual
attention. Such an improvement could be made through improved communication
during the dealings with patients. The feeling experienced and expressed was
that doctors have to pay more attention to patients' problems and share with
them their experience. Patients also illustrated that doctors were successful
in achieving reliability, responsiveness, assurance and empathy. Especially
considering that the mean results for all four dimensions were all high.
The major findings derived from the empirical research phase
in terms of patients' experience of service delivery of nurses relating to the
four dimensions of service quality, are subsequently indicated.
In terms of reliability, it is clear from the results obtained
that the majority of respondents were satisfied with their interactions with
nurses with regard to their reliability. Patients indicated that they were most
satisfied with the honesty of nurses and their ability to examine them
properly. Patients were however of the opinion that there was room for
improvement in the way nurses acted in their best interests, and how such
action resulted in a trust patients have towards nurses. Such improvements
could be through improved compassion and understanding during the diagnoses of
the problem. Such an improvement could also enhance their satisfaction level
with the reliability of nurses.
In terms of responsiveness, the results indicated that the
majority of respondents were satisfied with their experience of nurses'
responsiveness. Respondents indicated that they were most satisfied with the
fact that nurses always listened to what they had to say and communicated the
prescription of medications for their treatment in a manner that they could
understand. Patients were however of the opinion that nurses could inform them
more about their state of health during consultation and respond more to
129
their queries. Such room for improvement could be through
improved communication during the diagnoses of the problem. The feeling was
that nurses had to develop more patience and understanding with patients whilst
diagnosing the patient.
In terms of assurance, it was evident that the majority of
respondents were satisfied with the dealings they had had with nurses with
regard to the nurses' assurance. Respondents indicated that they were most
satisfied with the fact that nurses respected the confidentiality of their
treatment, the fact that they carried out their tasks competently, and were
well trained and qualified. Respondents were however of the opinion that nurses
could show more respect and dignity towards them. Such an improvement could be
through improved work ethic in the hospital where patients could be treated
with more respect.
In terms of empathy, the results indicated that the majority
of patients were satisfied with the dealings they had had with nurses with
regard to the nurses' empathy. Patients indicated that that they were most
satisfied with the nurses' concerns about their wellbeing, the way they cared
for them, and the fact that they understood their specific needs. Patients were
however of the opinion that nurses could provide them with more individual
attention. Such an improvement could be made through improved communication
during the dealings with patients. The opinion of patients was that nurses have
to pay more attention to patients' problems and share with them their
experience.
Main conclusions
? The majority of patients were satisfied with their
interactions with doctors regarding their reliability, responsiveness,
assurance and empathy.
? The majority of patients were satisfied with their
interactions with nurses regarding their reliability, responsiveness, assurance
and empathy.
? Nurses were overall more successful in achieving
reliability, responsiveness, assurance and empathy compared to doctors.
? In terms of perceptions of the actual service delivery of
doctors on the service dimension, patients indicated that doctors were more
successful in achieving responsiveness and empathy compared to reliability and
assurance.
? In terms of perceptions of the actual service delivery of
nurses on the service dimension, patients indicated that nurses were more
successful in achieving empathy and assurance compared to responsiveness and
reliability.
130
? In terms of the comparison between perceptions of actual
service delivery of doctors and nurses on the service dimension, patients
indicated that nurses were overall more successful in achieving empathy,
assurance, responsiveness and reliability compared to doctors.
Implications
Executives at the military hospital need to implement service
quality programmes to educate medical personnel about the importance of service
quality in health care for patient retention and loyalty.
Recommendations
Patient satisfaction is perceived as a vital aspect for the
military hospital. Not only to satisfy patient needs, but to increase patient
loyalty. Patient loyalty is an essential aspect in terms of increasing market
share and profitability. The recommendations for this section are based on the
results of the empirical findings in terms of patients' rating of doctors and
nurses on the service quality dimensions.
In terms of the doctors' services, patients felt a need for
more privacy in terms of the confidentiality of their treatment, a need for
more individual attention, a need to be heard, and to trust doctors. Therefore,
such needs could be addressed through improved compassion, communication and
understanding of doctors during the diagnoses of the problem. The feeling was
expressed that doctors should pay more attention to patients' problems and
share with them their experience. Doctors at the military hospital should
develop more work ethic where patients' records and cases should never be
discussed with anyone without patients' permission. The military hospital
should employ highly trained and qualified doctors to address the trust issue
in patients. Lastly, consultation time may need to be reviewed to add some
extra time to better address patients' needs during their consultation with
doctors.
In terms of the nurses' services, patients felt a need for
more trust towards nurses, a need for more information, for more respect and
for more individual attention. Such needs could be addressed through improved
patience, compassion, communication and understanding of nurses during their
dealings with patients. Nurses should develop more work ethic where patients'
records and cases should never be discussed with anyone without their
permission. Officials in the hospital should hire highly trained and
131
qualified nurses to address the issue of trust in patients and
consultation time may need to be reviewed to add some extra time to better
address patients' needs during their dealings with nurses. Other hospitals
could enhance the reliability, responsiveness, assurance and empathy of their
doctors and nurses based on the above recommendations.
6.3 PATIENTS' PERCEPTIONS REGARDING THE TANGIBLE ASPECTS
AT A SPECIFIC MILITARY HOSPITAL
The secondary objective related to patients' perceptions
regarding the tangible aspects at a military hospital was illustrated as
followed:
? To establish the perception of patients regarding the
tangible aspects of a military hospital in Gabon.
The following hypothesis below resulted from the
above-mentioned secondary objective:
H05: Patients do not have a positive perception of the
tangible aspects of a military hospital in Gabon.
The major findings in terms of patients' perceptions regarding
the tangible aspects were as follows:
Patients have a positive perception of the tangible aspects of a
military hospital.
The tangible aspect of service quality is crucial in the
delivery of services in hospitals as it can reduce the gap between patients'
expectations and the actual delivery of service. It provides a picture of what
is inside a hospital and can influence patients' choice when selecting a health
service provider. Tangible aspects of service are viewed to significantly
influence patients' satisfaction level with services provided.
In addition to the main findings from the literature review,
the findings from the empirical study indicated that patients had a positive
perception of the tangible aspects of a military hospital. The empirical
results confirmed that the tangible aspect significantly influenced patient
satisfaction.
132
Main conclusion
The majority of patients indicated that they had a positive
perception of the tangible aspects of a military hospital.
Implication
The military hospital needs to maintain or improve the
tangible aspects of services provided, in order to create a higher level of
patient retention and loyalty.
Recommendations
It was concluded from the literature review that the tangible
aspect of services needs to be maintained and improved in order to ensure
patient satisfaction. The empirical results indicated some aspects that can be
improved, and this will form the basis for the recommendations. Patients
indicated that the interior decoration at the hospital and the furniture at the
hospital such as beds and chairs needed to be improved. Such improvement could
be through changing the furniture and the interior decoration at the hospital
on a regular basis. Other hospitals could enhance the tangible aspects of their
service through changing their equipment on a regular basis.
6.4 OVERALL PERCEPTION OF SERVICES AND FACTORS THAT COULD
INFLUENCE THE CHOICE OF A MILITARY HOSPITAL
Both the overall perception of the military hospital and the
factors that could influence the choice of a military hospital will guide the
management of the hospital in terms of areas of continued focus and
improvement. The patients indicated that they were content with the overall
service provided by the hospital and that they felt good about coming to the
hospital. Patients furthermore indicated that the quality of the doctors and
nurses working at the hospital, as well as the availability of modern medical
equipment, influenced their decision to visit the hospital.
Main conclusion
The majority of patients indicated that overall, the service
offering of the military hospital was superior to the one offered by government
hospitals.
133
Implication
The military hospital would need to maintain or improve its
current levels of service delivery to patients in order to create a higher
level of patient retention and loyalty.
Recommendation
It will be to the benefit of the military hospital if
management enhanced the quality of service delivery by the administrative staff
of the hospital. A strategy to enhance such service delivery is to invest more
capital in the training of administrative staff in areas such as people skills
(towards patients specifically), service delivery through the use of
technology, telephone communication skills, friendliness towards patients (i,e.
customer care), as well as knowledge regarding the administrative processes and
systems of the hospital. Furthermore, more robust recruitment practices must be
put in place to ensure that the most skilled and qualified individuals are
recruited for administrative positions, specifically. This will enhance the
service delivery levels of the administrative staff at the hospital, and the
satisfaction levels of patients, since they are interacting with more
knowledgeable and competent employees in administration, but also experience
and communicate the overall image and reputation of the hospital in the
community.
6.5 LIMITATIONS OF THIS STUDY
This study was exposed to various limitations like any other
research. However, future investigations on this type of research will be able
to generate new thoughts and provide a deeper understanding of service quality
in hospitals. The limitations in this study are outlined.
6.5.1 Limitations based on the literature
review
The literature review in this study indicated the major
constituents of service quality such as reliability, responsiveness, assurance,
empathy and tangibility and an understanding of the relationships between
service quality, customer satisfaction, loyalty and profitability. However, new
literatures may be necessary to provide deeper assessments of services
delivered by doctors and nurses respectively on each of their service quality
dimension.
134
6.5.2 Limitations of the empirical phase of
study
The research was done on service quality at the military
hospital in Libreville in Gabon and is specific to the hospital in question.
Thus the study is limited to that particular hospital and it cannot be applied
to the entire industry as the population chosen for the study was limited to
the said hospital only.
? Sampling is a problem, as there is no sample which can allow
the researcher to make forecasts of the entire population. In this current
study, a total of 200 respondents completed the survey questionnaires.
? The sample only included patients who were at least 18
years, males and females, who had experienced medical services and stayed over
at the military hospital for at least one night. Thus the study did not involve
all patients and it is not possible to make forecasts for all patients of the
military hospital in Libreville in Gabon.
6.6 RECOMMENDATIONS FOR FUTURE RESEARCH
The current study only assessed service quality at the
military hospital in Libreville in Gabon, thus it cannot be utilised for the
entire health care industry. A future study may be done to investigate service
quality for the entire industry and include multiple healthcare practices.
6.7 CONCLUDING REMARKS
Both the primary and secondary objectives formulated for this
study were addressed based on the conclusions, implications and recommendations
in this research. It is therefore concluded that the findings of this research
help to understand service quality in a military hospital setting.
135
REFERENCES
Aaker, K. (2006). Marketing Research, 9th edition.
California: Wiley.
Aaker, D.A., Kumar, V., Day, G.S., Lawley, M. & Stewart,
D. (2007). Marketing Research, 2nd edition, Milton, Qld: John Wiley
& Sons, Australia, Ltd.
Al Sharif, B. F. T. (2008). Patients' satisfaction with
hospital services at Nablus District, Westbank Palestine . Master's
Thesis, University of Palestine.
Angelis, J., De Lima, E.P. & Siraliova, J. (2010). Service
experiences: business and management implications. Current Issues of
Business, 5:6-23. Available from EBSCOHost: Business Source Premier:
http://search.global.epnet.com.
(Accessed 9 August 2010).
Babbie, E. & Mouton, J. (2009).The practice of social
research.1st edition. Cape Town: Oxford University Press.
Babin, B.J. & James, K.W. (2010). A brief retrospective
and introspective on value. European Business Review, Vol.22,
pp. 471-478.
Basheer, A., Al-Alak, A. & Alnaser, A.S.M. (2012).
Assessing the Relationship Between Higher Education Service Quality Dimensions
and Student Satisfaction. Australian Journal of Basic and Applied
Sciences, Vol.6 (2012), pp. 156-164.
Benlian, A., Koufaris, M. & Hess, T. (2012). Service
Quality in Software-as-a-Service: Developing the SaaS-Qual Measure and
Examining Its Role in usage Continuance. Journal of Management Information
Systems, Vol. 28, pp. 85-126.
Berndt, A. & Brink, A. (2008). Relationship marketing
and customer relationship management and customer service. Landsdowne:
Juta.
Bhasin, H. (2011). Services marketing mix. Available
from:
http://www.marketing91.
com/service-marketing-mix/ . (Accessed July 2012).
136
Bick, G., Abratt, R. & Möller, D. (2010). Customer
service expectations in retail banking in Africa. South African Journal of
Business Management, Vol. 41, (2010), pp.13 - 28.
Bodet, G. & Assolant, L. B. (2011). Consumer Loyalty in
Sport Spectatorship Services: The Relationships with Consumer Satisfaction and
Team Identification. Psychology and Marketing, Vol. 28(8), pp.
781-802.
Bogomolova, S. (2011). Service quality perceptions of solely
loyal customers. International Journal of Market Research, Vol. 53,
pp.793-810.
Bourgarel, M. (2010). Emerging viral threats in Gabon: health
capacities and response to the risk of emerging zoonotic diseases in Central
Africa. Emerging. Health Threats Journal, Vol.3 (2010), pp.1-112.
Brizee, A. (2010). Specialising in Rhetoric and
Composition, Professional writing, and Public Rhetorics. Doctoral Thesis,
Perdue University.
CAMES (Conseil Africain et Malgache pour l' Enseignement
Supérieur). (2012).
Available from :
http://www.guninetwork.org/guni.network/institutional-members/
strathmore-university-1.
(Accessed July 2012).
Cant, M., Gerber-Nel, C. & Kotze, T. (2005). Marketing
Research. 2nd edition.Claremont: New Africa Books.
CENAREST. (2011). Les editions du CENAREST. Available
from :
http://www.edi tions.cenarestgabon.com/.
(Accessed July 2012).
Chebat, J. C., Sirgy, M. J. & Grzeskowiak, S. (2010). How
can shopping mall management best capture mall image? Journal of Business
Research, Vol.63, pp. 735- 740.
Chirurgie générale. (2010). Hôpital
d'instructions des armées. Available from :
http://hia-obo.org/fr/serviceschirurgicaux.php.
(Accessed 2012).
137
Churchill, G.A. & Brown, T.J. (2007). Basic Marketing
Research. 6th edition. Ohio: Thomson South-Western.
Cockalo, D., Djordjevic, D. & Sajfert, Z. (2011). Elements
of the model for customer satisfaction: Serbian economy research. Total
Quality Management, Vol. 22, pp. 807- 832.
Conradie, E. S. (2011).The influence of internal marketing
elements on the brand awareness of car rental customers in South Africa.
Doctoral Thesis, University of Johannesburg.
Country Brief Gabon. (2010). Estandards forum Financial
Standards Foundation. Available from:
www.estandardsforum.org
(Accessed 12 July 2011).
Desai, V.V. (2011). Case Study: Patient satisfaction and
service quality dimensions. Journal of Advance Management, Vol. 4 (5)
May (2011), pp. 1-78.
Diehl, K. & Poynor, C. (2010). Great Expectations?!
Assortment Size, Expectations and Satisfaction. Journal of Marketing
Research, Vol. XLVII (2010), pp.312-322.
Doghaither, H.A.I., Abdelrhman, B.M., Saeed, A.A., Magzoub,
M.E.M.A. (2003). Factors influencing patient choice of hospitals in Riyadh,
Saudi Arabia. The Journal of the Royal Society for the Promotion of Health,
123(2):105-109.
Dosen, D. O. (2009). Perceptions among Croatian surgeons of
services marketing application to healthcare organisations. Journal of
Health Services Marketing, Vol. 21 (2009), pp.203-218.
Du Plessis, L. (2010). Customer relationship management
and its influence on customer loyalty at Liberty Life in South Africa.
Unpublished Master's Thesis, University of Johannesburg.
Fernandes, A.M. (2009). Structure and performance of the
service sector in transition Economies. The European Bank for
Reconstruction and Development Journal, Vol.2 (2009), pp.400-500.
138
Fornell, C., Rust, R.T. & Dekimpe, M.G. (2010). The Effect of
Customer Satisfaction on Consumer Spending Growth. Journal of Marketing
Research, Vol. XLVII, pp 28-35.
Forrest, V., Morgeson, L., Mithas, S., Timothy, L., Keiningham,
A. & Aksoy, L. (2011). An investigation of the cross-national determinants
of customer satisfaction. Journal of Marketing Sciences, Vol. 39
(2011), pp.198-215.
Gabon. (2010). Health indicators. Country Brief Review,
Vol.3 (2010), pp.1-13.
Gabon. (2011). African renaissance outlook. UNDP, UNECA
Review Paper, Vol.3 (2011), pp.1-55.
Gabon Economic Outlook. (2012). Available from:
www.africaneeconomicoutlook.
org/en/countries/central-africa/gabon/(Accessed 2012).
Gabon Poverty and Reduction Strategy Paper. (2012). Women and
children first. World Health Organisation Review, Vol.3 (2012),
pp.2-99.
Gilaninia, S., Almani, A.M., Pournaserani, A. & Mousavian,
S.J. (2011). Relationship Marketing: A New Approach to Marketing in the Third
Millennium. Australian Journal of Basic and Applied Sciences, Vol.
5(5), pp.787-799.
Global Health. (2012). Gabon healthcare system.
Available from:
http://www.globalsu
rance.com/resources/gabon/
(Accessed July 2012).
Golder, P.N., Mitra, D. & Moorman, C. (2012). What Is
Quality? An Integrative Framework of Processes and States. Journal of
Marketing, Vol. 76, pp. 1-23.
Greenstone, M. & Hanna, R. (2011). Environmental regulations,
air and water pollution, and infant mortality in India. Economics
Report, Vol. 1 (2011), pp.1-48.
Grewal, R. Chandrashekaran, M. & Citrin, A.V. (2010).
Customer Satisfaction Heterogeneity and Shareholder Value. Journal of
Marketing Research, Vol. XLVII, pp.612-626.
139
Grigoroudis, E. & Siskos, Y. (2012). Methods for
measuring and implementing service quality. New York: McGraw Hill
Education.
Grobbelaar, S.F. (2006). Measuring the impact of perceived
quality of service and price amongst restaurant customers in Johannesburg.
Master's Thesis, University of Johannesburg.
Grönroos, C. (2007). Service management and marketing:
Customer management in service competition.3rd edition.
England: John Wiley and Sons Ltd.
Hair, J., Bush, R. & Ortinau, D. (2006). Marketing
research within a changing environment. 3rd edition. New York: McGraw-Hill
Irwin.
Haseki, M.I. (2013). Customer expectations in mall restaurants: A
case study. International Journal of Business and Society, Vol. 14,
pp. 41 - 60.
Health. (2007). A healthy future. Gabon Spring
Review, Vol.2 (2007), pp.1-88.
Health and Safety in Gabon. (2011). Available
from:http://www.spainexchange.com/ guide/GA-health.htmd (Accessed 26
July 2011).
Heitzler, C. D., Asbury, L. D. & Kusner, S. L. (2008).
Bringing «play» to life: The use of experiential marketing in the
VERB campaign. American Journal of Preventive
Medicine, Vol.34 (6), pp. 188-193.
Hernandez, R.M.S., Tur, V.M., Peiro, J.M. & Ramos., J.
(2009). Testing a hierarchical and integrated model of quality in the service
sector: Functional, relational, and tangible dimensions. Total Quality
Management, Vol. 20, pp. 1173-1188.
Hill, N., Roche, G. & Allen, R. (2012). Customer
experience through the customer's eyes. London: Cogent Publisher.
Historique. (2010). Hôpital d'instructions des
armées. Available from: http://hia-obo.
org/fr/historique.php (Accessed 2012).
140
Hoffman, D., Bateson, J.E.G., Wood, E. & Alexandra, J. K.
(2006). Services marketing concepts, strategies and cases. United
Kingdom: South-Western Cengage EMEA.
Hoffman, K. D., Bateson, J.E.G., Wood., E.H. & Kenyon,
A.K. (2009). Services marketing: Concepts, strategies and cases.
London: South-Western Cengage Publisher.
Holder, S. M. (2008). Changes in physical evidence and the
perception of service quality of patients in a hospital facility. Master's
Thesis, University of Johannesburg.
Hôpital d' instructions des armées. (2011).
Présentation. Available from:
http://hia-obo.org/Pr%C3%A9sentation-42.html
(Accessed 25 July 2011).
Hossain, M. & Leo, S. (2009). Customer perception on
service quality in retail banking in Middle East: the case of Qatar.
International Journal of Islamic and Middle Eastern Finance and
Management, Vol.2 (4) (2009), pp.338-350.
Hu, Y.J. (2011). How brand equity, marketing mix strategy and
service quality affect customer loyalty: The case of retail chain stores in
Taiwan. The International Journal of Organizational Innovation, Vol.
4, Number 1, pp.59-74.
Ince, T. & Bowen, D. (2011). Consumer satisfaction and
services: insights from dive tourism. The Service Industries Journal,
Vol. 31(2008) ,pp. 1769-1792.
International Diabetes Federation. (2010). Country Summary
Table for 2010. Available from:
http://www.diabetesatlas.org/map
(Accessed in 2012).
Irani, F. (2008). Client satisfaction management in public
companies. Journal of Marketing, Vol. 63 (2008), pp. 33-44.
Jun, M. & Cai, S. (2010). Examining the relationships
between internal service quality and its dimensions, and internal customer
satisfaction. Total Quality Management Journal, Vol.21 (2010),
pp.205-223.
141
Jupiter, E. (2011). Marketing services definition.
Available from:
http://www.ehow. com/facts
6784044 marketing-service-definition.html (Accessed 2012).
Kapoor, R., Paul, J. & Halder, B. (2012). Services
marketing: Concepts and practices. New Delhi: McGraw Hill Education.
Kasper, H., Helsdingen, P.V. & Gabbott, M. (2006).
Services marketing management: A strategic perspective. 2nd
edition. England: John Wiley and Sons, LTD.
Kaura, V. & Datta, S.K. (2012). Impact of Service Quality on
Satisfaction and Loyalty: Case of Two Public Sector Banks. Journal of
Management, pp.65-76.
Kim, Y.K. (2008). A study on medical services quality and its
influence upon value of care and patient satisfaction: A Focus upon outpatients
in a large-sized hospital. Total Quality Management, Vol. 19 (2008),
pp. 1-1171.
Kumar, V., Petersen, J.A. & Leone, R.P. (2007). How valuable
is word-of-mouth? Harvard Business Review, 85(10):139-147.
Kyle, G. T. (2010). The effect of service quality on customer
loyalty within the context of ski resorts. Journal of Park and Recreation
Administration, Vol.18 (2010), pp. 3-4.
Laboratoire d'analyse médicales. (2010). Hôpital
d'instructions des armées. Available from :
http://hia-obo.org/fr/laboratoireanalysesmedicales.php
(Accessed 2012).
Laurant, M.G.H., Hermens, R.P.M.G., Braspenning, J.C.C.,
Akkermans, R.P., Sibbald, B. & Grol, R.P.T.M. (2008). An overview of
patients' preference for, and satisfaction with, care provided by general
practitioners and nurse practitioners. Journal of Clinical Nursing,
Vol.17, pp. 2690-2698.
Leke, A., Lund, S., Roxburgh, C. & Van Wamelen, A. (2010).
What is driving Africa's growth. Available from:
www.mckinsey.com/insights/economic
studies/whats africa growth
142
Leroy, E. & Gonzalez, J.P. (2012). Filovirus research in
Gabon and equatorial Africa: the experience of a research center in the heart
of Africa. Journal of Health, 4(9):159604.
Likert Scale. (2012). Likert Scale - What is it? When
to Use it? How to Analyze it? Available from: http: //
www.surveygizmo.com/survey-blog/likert-scale-what-is-it-how-to-analyze-it-and-when-to-use-it/
(Accessed November 2012).
Lings, I.N. & Greenley, G.E. (2009). The impact of
internal and external market orientations on firm performance. Journal of
Strategic Marketing, Vol.17 (1), pp.41-53.
Liu, X. & Homburg, C. (2007). Neglected Outcomes of
Customer Satisfaction. Journal of Marketing, Vol. 71 (2007), pp
.133-49.
Londre, L.S. (2010). Marketing, the Marketing Mix (4Ps), and
the Nine Ps. Journal of Marketing, Vol.3 (2010), pp.1-100.
Lovelock, C., Wirtz, J. & Chew, P. (2009). Essentials
of Services Marketing. New York: Prentice Hall.
Lovelock, C. & Wirtz, J. (2011). Services Marketing:
People, Technology, Strategy. Upper Saddle River. New Jersey: Prentice
Hall.
Malhotra, N.K. (2007). Marketing research an applied
orientation. New Jersey: Pear-son Prentice Hall.
Malhotra, N.K. (2009). Basic Marketing Research - A
Decision-Making Approach.3rd edition. Upper Saddle River, New Jersey:
Pearson Education.
Malhotra, N.K., Hall, J., Shaw, M. & Oppenheim, P.P.
(2008). Essentials of Marketing Research - An Applied Orientation. 2nd
edition. New South Wales: Pearson Education Australia.
Markovic, S. & Raspor, S. (2010). Measuring perceived
service quality using Serv-
qual: A Case Study of the Croatian Hotel Industry. Journal
of Management, Vol. 5, pp.195-209.
143
Médecine interne. (2010).Hôpital d'instructions
des armées. Available from:
http://hia
-obo.org/fr/medecineinterne.php
(Accessed 2012).
Mekoth, N., George, P.B., Dalvi, V., Rajanala, N. &
Nizomadinov, K. (2012). Service Quality in the Public Sector Hospitals: A Study
in India, Hospital Topics, Vol.90, pp.16-22.
Meng, J.G., Summey, J.H., Herndon, N.C. & Kwong, K.K. (2009).
Some retail service quality expectations of Chinese shoppers. International
Journal of Market Research, Vol. 51 (2009), pp. 773-796.
Mitra, D. & Fay, S. (2010). Managing service expectations in
online markets: A signalling theory of e-tailer pricing and empirical tests.
Journal of Retailing, Vol. 86 (2), pp. 184-199.
Mohammad, A.A.S. & Alhamadani, S.Y.M. (2011). Service quality
perspectives and customer satisfaction in commercial banks working in Jordan.
Middle Eastern Finance and Economics Journal, Vol 14 (2011),
pp.60-72.
Mosley, R. W. (2007). Customer experience, organisational culture
and the employer brand. Journal of Brand Management, Vol.15 (2007),
pp.123-134.
Munyaradzi, W.N. (2010). The mediating role of customer
relationship management on customer retention at selected motor vehicle
dealership in the Buffalo City Municipality. Master's Thesis, University
of Fore Hare, South Africa.
Naidoo, L.P. (2008). Internal marketing in a customer service
centre. Unpublished Master's dissertation. Johannesburg: University of
Johannesburg.
Naik, K.C.N. (2010). Service Quality (Servqual) and its Effect on
Customer Satisfaction in Retailing. European Journal of Social Sciences,
Vol.16 (2010), pp.1-600.
National Department of Health. (2006).Health Facility
Definitions. Journal of Health Science, Vol.2 (2006), pp.1-7.
144
Nejad, S.B., Allegranzi, B., Syed, S.B., Ellis, B. &
Pittet, D. (2011). Health-care-associated infection in Africa: a systematic
review. Bulletin of World Health Organisations, Vol.89 (2011),
pp.757-765.
Olusoji, D. (2009). Perception and patient satisfaction: A
case study of Olabisi Onabanjo University Teaching Hospital Sagamu,
Nigeria. MBA Thesis, Blekinge Institute of Technology, Nigeria.
Ophtalmologie. (2010). Hôpital d'instructions des
armées. Available from:
http://hia-obo.org/fr/ophtalmologie.php
(Accessed 2012).
Organe exécutif de la CEMAC. (2012). Available from:
http://www.oceac.org/details.
php?ref=main&rubrq=23&id=40 (Accessed 21 July 2012).
Orl & Ccf. (2010). Hôpital d'instructions des
armées. Available:
http://hia-obo.org/fr/orl-ccf.php
(Accessed 2012).
Orsingher, C., Marzocchi, G.L. & Valentini, S. (2011).
Consumer (Goal) Satisfaction: A Means-Ends Chain Approach. Psychology and
Marketing Journal, Vol. 28(7), pp.730- 748.
Parasuraman, A., Grewal, D. & Krishnan, R. (2007).
Marketing Research. 2nd edition. New Jersey: Houghton Mifflin
Company.
Pharmacie hospitalière. (2010). Hôpital
d'instructions des armées. Available from:
http://hia-
obo.org/fr/pharmaciehospitaliere-sterilisation.php
(Accessed 2012).
Pomering, A., Noble, G. & Johnson, L. (2011).
Conceptualising a contemporary marketing mix for sustainable tourism.
Journal of Sustainable Tourism, Vol. 19(8), pp.953-969.
Pradhan, S. & Roy, S. (2011). Determinants of Satisfaction
and Loyalty in Apparel Retailing. Journal of Marketing, Vol. 5,
pp.78-88.
145
Prescott, M.R. & Kruk, M.E. (2012). The Role of Health
Systems and Policies in Promoting Safe Delivery in Low- and Middle- Income
Countries: A Multilevel Analysis. American Journal of Public Health,
Vol.102 (2012), pp.645 to 650.
Programme Economique Régional de la CEMAC. (2009). Vers
une économie intégrée et émergente : Programme
économique régionale. Journal de l'Organisation Mondial de la
Santé, Vol.1 (2009), pp.1-30.
Proquest. (2007). Gabonese Republic. UN Development
Programme, Human Development Report, Vol.2 (2007), pp.1-4.
Prouse, S. (2011). Verbal communication with the author on 17
March. Johannesburg (Notes in possession of author).
Raboka, H.M. (2006). Determinants of customer satisfaction and
service quality: The case of Romanian public services. Transylvanian Review
of Administrative
Sciences, Vol.16 (2006), pp.124-135.
Radiologie et imagérie médicale. (2010).
Hôpital d'instructions des armées. Available from:
http://hia-obo.org/fr/Radiologieimageriemedicale.php
(Accessed 2012).
Rahman, M. & Miazee, H. (2010). E-Service Quality and
Customer Satisfaction: A Study of Online Customers in Bangladesh. Master's
Thesis, Mid Sweden University.
Rajasekhar, M., Muninarayanappa, M. & Reddy, S.V.S. (2009).
The GAP model analysis of service quality in Indian higher education. Asia
-Pacific Journal of Social Sciences, Vol.1 (2009), pp. 214-229.
Republic of Gabon. (2008). Project completion report health
services development. African Development Bank Review, Vol.1 (2008),
pp. 1-57.
Revere, L. (2010). How healthcare organisations use the internet
to market quality achievements. Journal of Healthcare Management,
Vol.3 (2010), pp.1-114.
146
Rezaei, M.D., Rezaei, H.K., Alipour, H. & Salehi, S.K.
(2011). Service quality, client satisfaction and client personality in the
public companies. Australian Journal of Basic and Applied Sciences,
Vol.5 (2011), pp.483-491.
Roberts-Lombard, M. (2006). Verhoudingsbemarking by
reisagentskappe in die Wes-Kaapprovinsie. Doctoral Thesis, Potchefstroom:
Noordwes-Universiteit.
Rohini, R.(2006). Service quality in Bangalor hospitals: An
Empirical study. Journal of Services Research, Vol.6 (2006), pp.
1-113.
Rootman, C. (2006). The influence of customer relationship
management on the service quality of banks. Unpublished Master's
dissertation. Port Elizabeth: Nelson Mandela Metropolitan University.
Rust, R.T. & Huang, M.H. (2012). Optimizing Service
Productivity. Journal of Marketing, Vol. 76.pp. 47-66.
Saunders, M., Lewis, P. & Thornhill, A. (2007). Research
Methods for Business Students. 4th edition.London. Pitman Publishing.
Savescu, R.F. (2011). Marketing mix in microcredit organisations.
Review of Management and Economic Engineering, Vol. 10 Issue 3,
p39-44.
Service d'accueil. (2010).Hôpital d'instructions des
armées. Available from:
http://hia-obo.org/fr/accueil-des-urgences.php
(Accessed 2012).
Services Marketing. (2012). Available from:
http://pdfworld.net/download.php?id=422
806 (Accessed July 2012).
Service Sector Around the World. (2012). Available from:
http://shodhganga.inflibnet
.ac.in/bitstream/10603/3077/9/09chapter%201.pdf (Accessed July
2012).
Shiu, Y.M. & Yu, T.W. (2010). Internal marketing,
organisational culture, job satisfaction, and organisational performance in
non-life insurance. The Service Industries Journal, Vol. 30 (2010),
pp. 793-809.
147
Siddiqui, M.H. & Sharma, T.G. (2010). Analyzing customer
satisfaction with service quality in life insurance services. Journal of
Targeting, Measurement and Analysis for Marketing, Vol. 18(2010), pp 221 -
238.
Siu, N.Y.M., Zhang, T.J.F. & Yau, C.Y.J. (2013). The Roles
of Justice and Customer Satisfaction in Customer Retention: A Lesson from
Service Recovery. Journal of Business Ethics, Vol. 114, pp.675-686.
Tan, C.W., Benbasat, I. & Cenfetelli, R.T. (2013).
IT-Mediated customer service content and delivery in electronic governments: An
empirical investigation of the antecedents of service quality. MIS
Quarterly, Vol. 37, pp. 77-109.
Temesgen, Z., Negi, R. & Ketema, E. (2010). An Assessment
of the Marketing Strategy for Mobile Services of Ethiopian Telecommunication
Corporation. Services Marketing Quarterly, Vol. 2, pp. 31:50-71.
Terre Blanche, M., Durrheim, K. & Painter, D. (2006).
Research in practice. 2nd edition. Cape Town: University of Cape Town
Press.
The Self-Administered Survey. (2012). Available from:
http://www.htm.uoguelph. ca/MJResearch/ResearchProcess/SelfAdministered.htm
(Accessed August 2012).
Trading Economics. (2012). Value added, annual percentage
growth in Gabon. Available from:
http://www.tradingeconomics.com/gabon/services-etc--value-added-annual-percent-growth-wb-data.html
(Accessed 2012).
Tsai, W.H., Hsu, W. & Lin, T.W. (2011). New financial
service development for banks in Taiwan based on customer needs and
expectations. The Service Industries Journal, Vol. 31, pp. 215-236.
Tustin, D.H., Ligthelm, A.A., Martins, J.H. & Van Wyk, H.
(2005). Marketing Research in Practice. Pretoria: Unisa Press.
148
US Department of State Travel Advisory. (2010).Travel
Advisory for Gabon. Available from:
http://travel.state.gov/travel/cis
pa tw/cis/cis 1120.html(Accessed 25 July 2011).
Vanniarajan, T. & Arun, B. (2010). Service quality in health
care centres: An empirical study. Global Management Review, Vol. 4
(2010), pp. 1-16.
Van Vuuren, T. (2011). Customer loyalty in an optometric
practice: A case study perspective. Master's thesis, University of
Johannesburg.
Verma, H.V. (2012). Services marketing: Text and
Cases.2nd edition. Dorling Kinders-sley (India): Pearson
Education in South Asia.
Vlasic, G. & Kesic, T. (2007). Analysis of Consumers'
Attitudes toward Interactivity and Relationship Personalization as Contemporary
Developments in Interactive Marketing Communication. Journal of Marketing
Communications, Vol.13 (2007), pp.109-129.
Vrontis, D., Thrassou, A. & Zin, R.M. (2010). Internal
marketing as an agent of change - implementing a new human resource information
system for Malaysian Airlines. Journal of General Management, Vol. 36
(2010), pp.1-90.
Webster, C. & White, A. (2009). Exploring the national and
organizational culture within service firms. Journal of the Academic
Marketing Sciences, Vol. 38 (2010),pp. 38:691.
World Bank. (2006). From Disintegration to Reintegration: Eastern
Europe and the Former Soviet Union in International Trade. Global Economic
Development Review, Vol.3 (2006), pp.1-7.
World Bank. (2008). Unleashing Prosperity: Productivity Growth in
Eastern Europe and the Former Soviet Union. Global Economic Development
Review, Vol.6 (2008), pp. 210.
World Health Organisation. (2007). The right to Health.
Available from: http://www. who.int/mediacentre/factsheets/fs323/en/.
149
World Health Organisation. (2007). Survey on migration of health
workers in the African region. Health Care Review, Vol.2 (2007), pp.
19-23.
World Bank Development Indicators. (2012). Development
indicators. Social Sciences Report, Vol. 6 (2012), pp. 1-8.
Yesilada, F. & Direktor, E. (2010). Health care service
quality: A comparison of public and private hospitals. African Journal of
Business Management, Vol. 4(6) (2010), pp. 962-971.
Youl Ha, H. (2006). An integrative model of consumer satisfaction
in the context of e-services. International Journal of Consumer
Studies, Vol.30 (2006), pp.137-149.
Zainuddin, N., Previte, J. & Russell-Bennett, R. (2011). A
social marketing approach to value creation in a well-women's health service.
Journal of Marketing Management, Vol. 27, pp. 361-385.
Zeithaml, V.A. & Bitner, M.J. (2007). Services Marketing.
Integrating Customer Focus Across the Firm. New edition. New York:
McGraw-Hill/Irwin.
Zeithaml, V.A., Bitner, M.J. & Gremler, D.D. (2006).
Services marketing: Integrating customer focus across the firm.
Singapore: McGraw-Hill.
Zhang, L., Liu, B. & Ren, H. (2013). The personality profile
of excellent nurses in China: The 16PF. Journal of Health, Vol.43,
pp.219-224.
Zikmund, W.G. & Babin, B.J. (2007). Essentials of
marketing research. 3rd edition. Mason: Thomson South-Western.
150
APPENDIX A: COVERING LETTER
Comparing service quality of doctors and nurses at a
military hospital Dear respondent,
This questionnaire is built to obtain answers from you
regarding your perceptions and expectations of the quality of services offered
by doctors and nurses at the military hospital. This research will be used as
part of my studies with the University of Johannesburg.
This survey will remain confidential and anonymous and request
your honest answers.
Please feel free to answer at your own choice with an X
(cross) in the appropriate box where applicable.
This survey will take no longer than 10 minutes to complete.
Thank you for your time in completing this questionnaire.
Comparer la qualité des services offerts
par les médecins et le personnel infirmier dans un hôpital
militaire
Ce questionnaire est conçu pour obtenir des
réponses auprès de vous au sujet de vos perceptions et attentes
de la qualité des services offerts par les médecins et le
personnel infirmier à l'hôpital militaire.
Cette recherche sera utilisée dans le cadre de mes
études à l'Université de Johannesburg.
Cette enquête restera confidentielle et
anonyme.
Veuillez indiquer par un X dans le cadre
réservé à votre réponse. Ce formulaire ne vous
prendra pas plus de 10 minutes à compléter
Ponce Kokou Prof Roberts-Lombard, Mornay and
Dr Estelle Van Tonder
Student Research supervisors
Department of Marketing Management University of Johannesburg
Tel: 011 559 3031
APPENDIX B: QUESTIONNAIRE
|
Screening question: (Question de vérification)
Have you received services from the military hospital?
(Haviez-vous reçu des services de l'hôpital
militaire?)
|
Yes (oui) No (non)
|
Section A : Demographic profile(Profile
démographique)
1. Gender(sèxe):
3. Age (age):
151
Male (masculin)
5. Highest educational level (niveau
d'éducation):
6. Marital status (statue conjugal):
7. Employment level (forme d' emploi):
18
|
- 28
|
1
|
|
29
|
- 38
|
2
|
|
39
|
- 49
|
3
|
|
50
|
- 60
|
4
|
|
70 and above (plus de 70)
|
5
|
|
No formal education (aucune éducation)
|
1
|
|
Primary education (niveau primaire)
|
2
|
|
Secondary education (niveau secondaire)
|
3
|
|
Tertiary education (éducation
supérieure
|
4
|
|
Single (célibataire)
|
1
|
|
Married (marié(e)
|
2
|
|
Divorced (divorcé(e)
|
3
|
|
Widowed (veuf(ve)
|
4
|
|
Cohabitant(cohabitant)
|
5
|
|
Employed full-time (employé à temps
plein)
|
1
|
|
Employed part-time (employé à temps
partiel)
|
2
|
|
Self-employed in formal
sector(employé à titre personnel dans le
secteur formel)
|
3
|
|
Self-employed in informal sector (employé à
titre personnel dans le secteur informel)
|
4
|
|
Unemployed (sans emploi)
|
5
|
|
Student (étudient)
|
6
|
Pension (old age ) (retraité) 7
6. Residential area (lieu de résidence?):
7. First time patient? (est-ce votre première visite
dans cet hôpital?) :
|
In Libreville (dans la commune de
|
1
|
|
Libreville)
|
|
|
Outside of Libreville (hors de la commune de
Libreville)
|
2
|
|
Yes (oui)
|
1
|
|
No (non)
|
2
|
8. Required to stay over for at least one night?
(Etes-vous obligé de passer au moins une nuit dans
cet hôpital?) :
152
Section B: Below are list of points describing your
PERCEPTIONS of the military hospital services (Ci-dessous se trouve la
liste des éléments décrivant vos PERCEPTIONS des services
offerts à l'hôpital militaire)
Please indicate your level of agreement with an X, using the
following scale:
1=Strongly disagree, 2=Disagree, 3=Disagree somewhat,
4=Neutral, 5= Agree somewhat, 6= Agree, 7= Strongly agree
(Veuillez indiquez votre niveau de satisfaction par un X, en
utilisant l'échelle ci-dessous)
1= Très en désaccord, 2= En désaccord,
3= Un peu en désaccord, 4= Neutre, 5= Un peu d'accord, 6=D'accord,
7=Très d'accord)
I believe the medical doctors /nurses who treated me... (Je
crois que les médecins / infirmières qui m'ont
traité...)
|
Doctors(Médecins)
|
RELIABILITY(FIABILITE)
|
Nurses(Infirmières)
|
|
1
|
2
|
3
|
4
|
5
|
6
|
7
|
acted in a way that caused me to trust them (ont agi d'une
manière que j' ai développé une confiance en
eux/elles)
|
1
|
2
|
3
|
4
|
5
|
6
|
7
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
acted in my best interests (ont agi dans mes
intérêts personnels)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
had the ability to examine me properly
(avaient la capacité de m'examiné
correctement)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
were always honest with me
|
|
|
|
|
|
|
|
153
|
|
|
|
|
|
|
(ont été honnêtes envers moi)
|
|
|
|
|
|
|
|
|
1
|
2
|
3
|
4
|
5
|
6
|
7
|
RESPONSIVENESS(REACTIVITE)
|
1
|
2
|
3
|
4
|
5
|
6
|
7
|
|
|
|
|
|
|
|
informed me of my state of health during consultation
(m'ont informé de mon état de santé lors
de la consultation)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Communicated the prescription of medications for my treatment
with me in a manner that I could understand (ont communiqué avec moi
de manière à ce que je comprenne les prescriptions
médicales pour mon traitement)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
always responded to my queries (répondaient toujours
à mes questions)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
always listened to what I had to say (faisaient toujours
attention à ce que j'avais à dire)
|
|
|
|
|
|
|
|
|
1
|
2
|
3
|
4
|
5
|
6
|
7
|
ASSURANCE(ASSURANCE)
|
1
|
2
|
3
|
4
|
5
|
6
|
7
|
|
|
|
|
|
|
|
showed respect and dignity towards me
(m'ont traité avec beaucoup de respect)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
carried out their tasks competently (m'ont traité avec
beaucoup de compétence)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
respected the confidentiality of my treatment
(ont respecté la confidentialité de mon
traitement)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
were well trained and qualified (avaient beaucoup
d'expertise)
|
|
|
|
|
|
|
|
|
1
|
2
|
3
|
4
|
5
|
6
|
7
|
EMPATHY (EMPATHIE)
|
1
|
2
|
3
|
4
|
5
|
6
|
7
|
|
|
|
|
|
|
|
provided me with individual attention
(m'ont accordé une attention
particulière)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
were concerned about my wellbeing
(m'ont montré beaucoup d'intérêts pour
mon bien-être)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
understood my specific needs (ont compris mes besoins
personnels)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
cared about me
(ont pris soin de moi)
|
|
|
|
|
|
|
|
154
Section C: Tangibility statements (Affirmations
générales)
Please indicate your level of agreement with an X, using the
following scale:
1=Strongly disagree, 2=Disagree, 3=Disagree somewhat, 4=Neutral,
5= Agree somewhat, 6= Agree, 7= Strongly agree
(Veuillez indiquez votre niveau de satisfaction par un X, en
utilisant l'échelle ci-dessous
1= Très en désaccord, 2= En désaccord,
3= Un peu en désaccord, 4= Neutre, 5= Un peu d'accord, 6=D'accord,
7=Très d'accord)
I believe...
(Je crois que...)
|
TANGIBILITY(Aspect tangibles)
|
1
|
2
|
3
|
4
|
5
|
6
|
7
|
|
The furniture at the hospital such as beds and chairs was
comfortable
(le mobilier de l'hôpital tel que les lits et chaises
était confortable).
|
|
|
|
|
|
|
|
|
The interior decoration at the hospital was aesthetically
appealing
(J'ai aimé le décor interne de
l'hôpital).
|
|
|
|
|
|
|
|
|
The hospital had a pleasant atmosphere (J'ai aimé la
sensation atmosphérique de l'hôpital)
|
|
|
|
|
|
|
|
|
The colour scheme at the hospital was attractive (les
couleurs de l'hôpital étaient attirantes)
|
|
|
|
|
|
|
|
|
The toilet facilities in the hospital were clean (Les
toilettes étaient propres)
|
|
|
|
|
|
|
|
Section D: Overall perceptions of the services received
from the hospital (Vos perceptions générales des services
reçus de l'hôpital)
Using the scale provided, please indicate with an X, your overall
perceptions of services received the hospital
1=Strongly disagree, 2=Disagree, 3=Disagree somewhat, 4=Neutral,
5= Agree somewhat, 6= Agree, 7= Strongly agree
(Veuillez indiquez par un X en utilisant l'échelle
ci-dessous, vos perceptions générales de la qualité des
services reçus)
1= Très en désaccord, 2= En désaccord,
3= Un peu en désaccord, 4= Neutre, 5= Un peu d'accord, 6=D'accord,
7=Très d'accord
155
I believe...
(Je crois que...)
|
1
|
2
|
3
|
4
|
5
|
6
|
7
|
|
The overall quality of the administration service at the
hospital was excellent
(le service administratif de l'hôpital
était
excellent)
|
|
|
|
|
|
|
|
|
The overall service provided by the hospital was of a high
standard
(le service offert par l'hôpital était en
général de grande qualité)
|
|
|
|
|
|
|
|
|
The overall service I received at the hospital met my
expectations
(les services reçus de l'hôpital ont
coïncidé avec mes espérances)
|
|
|
|
|
|
|
|
|
I felt good about coming to this hospital for my treatment
(je me suis bien senti(e) dans cet hôpital)
|
|
|
|
|
|
|
|
|
Overall, the service offering of this hospital was superior to
the one offered by government's hospitals
(les services offerts dans cet hôpital
étaient meilleurs que ceux offerts par les hôpitaux
publiques)
|
|
|
|
|
|
|
|
Section E: Below are a list of factors which could
influence your decision to choose this hospital (En dessous, se trouve la
liste des facteurs qui pourraient influencer votre décision de choisir
cet hôpital)
Using the scale provided, please indicate with an X, how
influential these factors were in your decision to choose this hospital
1=Not at all important, 2=Low importance, 3=Neutral, 4=Moderately
important, 5=Extremely important
(Veuillez indiquer par un X, l'importance des facteurs
ci-dessous dans votre choix pour cet hôpital
1=Pas du tout important, 2= Peu d'importance, 3= Neutre, 4=
D'importance modérée, 5= Extrêmement important),
|
1
|
2
|
3
|
4
|
5
|
|
Availability of modern medical equipment
(La présence d'un équipement médical
moderne)
|
|
|
|
|
|
|
Specialised physicians
(Les médecins spécialisés)
|
|
|
|
|
|
|
Quality of nurses
|
|
|
|
|
|
|
(La qualité des infirmières)
|
|
|
|
|
|
|
|
Availability of medicines
(La disponibilité des medicaments)
|
|
|
|
|
|
|
|
Relatives living in the hospital area
(Un membre familial vivant à proximité de
l'hôpital)
|
|
|
|
|
|
|
|
Hospital near residence
(La proximité de l'hôpital du lieu de
résidence)
|
|
|
|
|
|
|
|
Ease of getting to hospital location (L'accès facile
à l'hôpital)
|
|
|
|
|
|
|
|
Care cost
(Le coût des soins hospitalier)
|
|
|
|
|
|
|
|
Patient's past experience
(L'expérience passée du patient)
|
|
|
|
|
|
|
|
Competent staff
(La compétence du personnel médical)
|
|
|
|
|
|
|
|
Know people who went to the hospital
(Connaissiez-vous des personnes ayant
fréquenté cet
auparavant ?)
|
hôpital
|
|
|
|
|
|
|
Good reputation in media
(la bonne renommée de l'hôpital)
|
|
|
|
|
|
|
|
Hospital cleanliness (l'hôpital est propre)
|
|
|
|
|
|
|
|
Employees are friendly towards patient (le personnel est
amical)
|
|
|
|
|
|
|
|
Hospital is well organised (l'hôpital est bien
organisé)
|
|
|
|
|
|
|
|
Other (autres)
|
|
|
|
|
|
|
Thank you
156
157
APPENDIX C: CONFIRMATION OF LANGUAGE
EDITING
Elsabeth Marnitz
10TH January 2014
TO WHOM IT MAY CONCERN
I, ELSABETH MARNITZ, hereby declare that the MINOR DISSERTATION
submitted in partial fulfilment of the requirements for the degree MAGISTER
COMMERCII in BUSINESS MANAGEMENT at the UNIVERSITY OF JOHANNESBRUG of
PONCE KOKOU with the title
SERVICE QUALITY AT A MILITARY HOSPITAL
has been language edited by me.

ELSABETH MARNITZ
720004392 (University of Johannesburg) Cell: 083 501
1545
| 

