I.1.6. Etiological of disorders of
glycemia
Etiological types designate defects, disorders or processes
that often result in diabetes
I.1.6.1. Type 1
diabetes
 fi fi
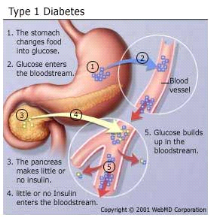
Figure 2 : Type 1 Diabetes mellitus
(Harris et al., 2003)
Type 1 indicates the processes of ß-cell destruction
that may ultimately lead to diabetes mellitus in which insulin is required for
survival to prevent the development of ketoacidosis, coma and death. Type 1 is
usually characterized by the presence of anti-glutamic acid decarboxylase
(anti-GAD) antibodies, islet cell or insulin antibodies which identify the
autoimmune processes that lead to ß-cell destruction. Consequently, the
pancreas secretes little or no insulin (Thunander et al.,
2008). Most cases are primarily due to T-cell mediated pancreatic
islet â-cell destruction, which occurs at a variable rate, and becomes
clinically symptomatic when approximately 90% of pancreatic beta cells are
destroyed (Craig et al., 2009). When the clinical
presentation is typical of type 1 diabetes but antibodies are absent, then the
diabetes is classified as Type 1B (idiopathic). Most idiopathic cases are of
African or Asian ancestry; however other forms of diabetes should also be
considered (Dunger et al., 2004).
I.1.6.2. Type 2 diabetes
mellitus
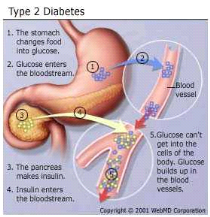
Figure 3 : Type 2 Diabetes mellitus
(Harris et al., 2003)
This form of diabetes, which accounts for 90-95% of those with
diabetes, previously referred to as non-insulin-dependent diabetes, type II
diabetes, or adult-onset diabetes, encompasses individuals who have insulin
resistance and usually have relative (rather than absolute) insulin deficiency
(Harris et al., 2003). Patients with type 2 diabetes
generally are older, although there is an alarming increase in the incidence of
type 2 diabetes in children and adolescents." Patients with type 2 diabetes
have insulin resistance syndrome (e.g., central obesity, hypertension,
hyperlipidemia) for many years (Harris et al., 2003).
There are three major pathophysiological abnormalities in patients with type 2
diabetes, that include early loss of first-phase insulin production associated
with defective beta cell secretion, peripheral resistance to insulin action
primarily in muscle tissue and the liver, and excessive hepatic
glucose production as disease progresses. Normally, first-phase insulin
secretion exerts an inhibitory effect on hepatic glucose production and output.
When a patient has beta cell defects, first-phase insulin secretion is impaired
and eventually lost, which results in fasting hyperglycemia (Hadi
et al., 2007).The body's attempt to moderate blood glucose
levels results in enhanced second-phase insulin secretion, and hyperinsulinism
occurs. Beta cells may secrete high levels of insulin to normalize blood
glucose levels and successfully maintain normoglycemia for many years.
Gradually, however, the beta cells may begin to falter, and insulin secretion
decreases. As hepatic glucose production increases, both fasting and
postprandial glucose levels become elevated (Hadi et al.,
2007).
Insulin resistance implies that the body's cells (insulin
receptors) are less sensitive to the action of insulin. Insulin
resistance, defined as the decreased ability of insulin to promote glucose
uptake in skeletal muscle and adipose tissue and to suppress hepatic glucose
output, may be present for many years before the development of any abnormality
in plasma glucose levels (Haffner, 2003). Consequently, blood
glucose levels rise, even though the beta cells produce more insulin. In
patients with insulin resistance, however, hyperinsulinemia does not suppress
gluconeogenesis, and chronic hyperglycemia develops. Insulin sensitivity can
decline by at least 70% before fasting plasma glucose concentrations become
abnormal, and it may take up to 20 years to reach that point (Haffner,
2003). Experts are not certain yet about the mechanism underlying
insulin resistance, but they know that obesity, particularly central obesity,
increases insulin resistance. They further speculate that defects in
intracellular signalling prevent glucose from entering cells
(Mukhyaprana et al., 2004).
Major risk factors for type 2 diabetes
mellitus
- Family history of diabetes (i.e., parents or siblings with
diabetes)
- Body Mass Index (BMI) (BMI > 27 kg per m')
- Radethnicity (e.g., African American, Hispanic, Native
American, Asian American, Pacific Islander) Age 45 years
- Previously identified impaired fasting glucose or impaired
glucose tolerance
- Hypertension (i.e. = 140/90 mm Hg)
- High-density lipoprotein cholesterol level I < 35 mg per
dL (0.9 mmol per L) or a triglyceride level = 250 mg per dL (2.83 mmol per
L)
- History of gestational diabetes mellitus or delivery of
babies above 4.032 g (Mukhyaprana et al.,
2004).
| 

