|

MINISTRY OF HIGHER EDUCATION REPUBLIC OF
CAMEROON
* * * * * * * * * * * *
THE UNIVERSITY OF BUEA PEACE-WORK-FATHERLAND
* * * * * * * * * * * *

FACULTY OF HEALTH SCIENCES
Department of
Nursing

PATIENT SATISFACTION WITH INTRAPARTUM
AND POSTPARTUM NURSING CARE :
THE CASE OF BUEA REGIONAL HOSPITAL
ANNEX
A DISSERTATION SUBMITTED IN PARTIAL FULFILLMENT OF
THE
REQUIREMENTS FOR THE AWARD OF A BACHELOR OF NURSING
SCIENCE (BNS)
DEGREE.
CHWINUI NGWINGMECHI MBEINKONG
UB 029154
Supervisor: Dr. NDE FON Peter
BUEA, July 2010.

CERTIFICATION.
This is to certify that the Research work «Patient
Satisfaction with Intrapartum and Postpartum Nursing Care» carried out in
the Buea Regional Hospital Annex was done by CHWINUI NGWINGMECHI MBEINKONG and
meets the criteria for the award of a Bachelor Degree in Nursing Science.
Sign: Sign:
Dr. Nde Fon Peter Chief Ndeso Atanga
Supervisor Head of Department
Sign:
Pr. Peter Martins NDUMBE
Dean of Faculty
DEDICATION
This piece of work is dedicated to all Nurses who have
the God-given
Assignment of caring for the Sick.
ACKNOWLEDGEMENTS
This research work would definitely not have been brought to
light without the restless efforts of several personalities. I will like to
appreciate all of you who built a step in one way or the other for me to climb
to the top of this mountain: Special thanks to my Lord and Saviour Jesus Christ
who gave me salvation and a reason to live.







A million thanks to my supervisor Dr. Nde Fon Peter for the
sleepless nights in directing and correcting this piece of work.
Many thanks go to my lecturers Chief Ndeso Atanga, Dr. Mrs Mary
Bih suh, Dr Palle John and Mr Sab Clement for all their guidance.
Innermost gratitude goes to my family: to my lovely parents
Mr and Mrs Ghogomu MBEINKONG for their unfailing love and tender
care. To my caring sisters Yehyeh, Nuigo, Keinui and my dear brother Halle for
their love.
Sincere thanks go to my lovely niece Pearl Ciana for the love she
gave me through out my stay in Yaounde.
Heartfelt thanks to my special friend Edwin for all his
assistance.
I must recognize the love and support of my friends Alvina,
Calvin, Betrand, Kelvina and Lesley for their support and to all my classmates
who made UB a place to be during my 4 years of study.
To the staff of the Buea Regional Hospital Annex Maternity, for
all your collaboration, I say THANK YOU.
LIST OF ABBREVIATIONS
A/L Advanced Level
AAP American Academy of Paediatrics
ACOG American College of Obstetricians and
Gynaecologists AIDS Acquired Immune Deficiency Syndrome
AMTSL Active Management of Third Stage of
Labour
BRHA Buea Regional Hospital Annex.
C/S Caesarean Section
DIVC Disseminated Intravascular Coagulation
EFW Estimated Foetal Weight
FH Fundal Height
FSH Follicle Stimulating Hormone
FSLC First School Leaving Certificate
HIV Human Immunodeficiency Virus
O/L Ordinary Level
TB Tuberculosis
WHO World Health Organization
LIST OF TABLES
Table 1: The Bishop Scoring System 21
Table 2: Distribution according to Age 37
Table 3: Distribution according to Levels of Education 38
Table 4: Distribution according to Profession 39
Table 5: Distribution according to Marital Status 40
Table 6: Distribution according to Number of days spent at
Maternity 40
Table 7: Distribution according to Parity 41
Table 8: Mode of Delivery 41
Table 9: Distribution according to Nurses' Attitude on Admission
42
Table 10: Distribution according to Nursing Comfort Measures
42
Table 11: Distribution according to Breathing Techniques Taught
43
Table 12: Distribution according to Environmental Hygiene 43
Table 13: Distribution according to Time spent with patients
43
Table 14: Distribution according to Interpretation of Patients'
feelings 44
Table 15: Distribution according to Monitoring Vital signs 44
Table 16: Distribution according to Patient Education 45
Table 17: Distribution according to Examination of Baby 46
Table 18: Distribution according to Examination of Mother 46
Table 19: Rating during Intrapartum (using the Likert's Scale)
47
Table 20: Rating during Postpartum(using the Likert's Scale)
48
Table 21: Patients' Recommendation of the Maternity 49
Table 22: Patients' Opinion on how satisfaction can be improved.
50
LIST OF FIGURES
Figure 1: Spontaneous Symphysiotmy 18
Figure 2: Estimated Foetal Weight 20
Figure 3: Intramuscular administration of Oxytocin 24
Figure 4: Deliverance of the placenta 25
Figure 5: Examining the placenta 25
Figure 6: Sketch diagram of BRHA 32
Figure 7: Organigram of BRHA 33
Figure 8: Distribution according to Age 47
Figure 9: Distribution according to Levels of Education
48
Figure 10: Distribution according to Professional 49
Figure 11: Distribution according to Marital Status
50
Figure 12: Distribution according to Number of days
spent at Maternity 51
Figure 13: Distribution according to Gravidity 52
Figure 14: Distribution according to Mode of Delivery
52
Figure 15: Distribution according to Patient Education
56
Figure 16: Rating during Intrapartum 58
Figure 17: Rating during Postpartum 59
Figure 18: Patients' Recommendation of the Maternity
60
Figure 19: Data Entry Form 64
TABLE OF CONTENTS
CERTIFICATION i
DEDICATION ii
ACKNOWLEDGEMENTS iii
LIST OF ABBREVIATIONS iv
LIST OF TABLES v
LIST OF FIGURES vi
TABLE OF CONTENTS vii
ABSTRACT ix
CHAPTER 1: INTRODUCTION AND
OBJECTIVES
1.0. Introduction 2
1.1. Background 3
1.2. Problem statement 4
1.3. Objectives of the study 5
1.4. Research questions 5
1.5. Hypothesis 5
1.6. Purpose of study 5
1.7. Justification 6
1.8. Limitations of the study 6
1.9. Operational definition of terms 7
CHAPTER 2: LITERATURE REVIEW
2.0. AN OVERVIEW OF LABOUR, DELIVERY AND POSTPARTUM 9
A. Introduction 9
B. Normal Labour and Delivery (Intrapartum) 9
C. The Postpartum Period (Puerperium) 12
2.1. NURSING CARE AND RESPONSIBILITIES 19
A. Introduction 19
B. Nursing role during labour and delivery 19
C. Nursing role during the postpartum period 26
2.2. PATIENTS' PERCEPTION ON NURSING CARE 29
Patient Satisfaction with Intrapartum and Postpartum Nursing
Care: Buea Regional Hospital Annex.
CHAPTER 3: METHODOLOGY
3.1. Study design 32
3.2. Study period: 32
3.3. Study site 32
3.4. Study population 34
3.5. Sampling method 34
3.6. Sample size 34
3.7. Data collection procedure 34
3.8. Ethical considerations 35
3.9. Budget 35
CHAPTER 4: PRESENTATION AND ANALYSIS OF
RESULTS
4.1 Socio-Demographic Data 37
4.2. Intrapartum Nursing Care Assessment 42
4.3. Postpartum Nursing Care Assessment 44
4.4. Assessment of Patient Satisfaction 47
4.4.1. Rating during Intrapartum (using the Likert's Scale)
47
4.4.2. Rating during Postpartum(using the Likert's Scale)
47
4.5. Patients' Recommendation of the Maternity 49
4.6. Patients' Opinion on how satisfaction can be improved. 50
CHAPTER 5: DISCUSSION, CONCLUSION AND
RECOMMENDATIONS
5.0. Introduction 52
5.1. Discussion of results 52
5.2. Conclusion 58
5.3. Recommendations 59
REFERENCES
APPENDIX
ABSTRACT
This research project «Patient Satisfaction with
Intrapartum and Postpartum nursing care the case of Buea Regional Hospital
Annex» was conceived due to the fact that nursing care is hardly
evaluated and so rarely improved on. This research aims at evaluating nursing
care by assessing patient satisfaction with nursing care offered.
It is a descriptive study targeting patients in the postpartum
ward who either had a normal delivery or an emergency caesarian section in the
BRHA maternity. Data was collected using a structured questionnaire which was
self-administered to a convenient sample of 37 participants.
The study revealed that the nursing care offered during
intrapartum was average but was poor during postpartum. Majority of the ratings
for patients' satisfaction during intrapartum (42.3%) were good implying that
the patients were fairly satisfied; while a majority of the ratings during
postpartum (37.6%) were poor implying that they were unsatisfied with the care.
A majority (52.8%) of the population somewhat agreed to recommend the maternity
services based solely on the nursing care they received. This therefore means
that the participants were fairly satisfied with the care offered in this
maternity.
Nurses therefore must improve on the care offered during labour
and delivery (intrapartum) and strive to provide adequate and standard care to
the postpartum mothers.
INTRODUCTION AND OBJECTIVES
1.0. INTRODUCTION
Health is not the mere absence of disease and infirmity but a
state of complete physical, social and mental wellbeing of an individual and
should be a universal human right [1]. Better health care outcomes will
therefore include social aspects of pregnancy and childbirth [2]. A good
outcome should be that every woman should be satisfied with the care and
support she received during pregnancy, delivery and postpartum periods and to
feel that she and her baby have been the center of care [3].
For many a woman, labour and childbirth is a time of
excitement and anticipation alongside uncertainty, anxiety, fear, and pain. The
memories and experience of childbirth remain with the woman throughout her
life. Clearly, the support and care they receive during this period is critical
[4].
Nurses have an important, enabling role to help the woman
during childbirth. There must be a high percentage of interpersonal skills in
the care of the woman in addition to being technically competent [5].
Postpartum period is significant for two important things: It
is a time for physiological adjustments for both the mother and her baby; and a
period of important social and physiological adjustments [6]. An emphasis on
individualized client-driven postpartum teaching including self-care and
newborn care is essential. Nursing care here should be flexible and organized
in collaboration with the woman to address her individual needs [3].
Evaluation is one of the most critical phases of the nursing
process because it supports the basis of the usefulness and effectiveness of
nursing practice. Nursing practice is patient-driven and patient-centered.
Accordingly, patient satisfaction has been strongly advocated for by nursing
professionals worldwide to be an important indicator of quality nursing care
delivery [7].
The purpose of measuring satisfaction here is to understand
the patients' experience of labour and childbirth and access postpartum care in
order to obtain information about the quality of nursing care and identify
problem areas.
1.1. BACKGROUND
In accordance with international professional standards and
guidelines, contemporary maternity care providers strive to create a childbirth
experience that is safe for the mother and her baby which is positive and
satisfying for the childbearing woman [8]. Researchers have focused on
identifying factors that promote a positive experience. Beneficial outcomes of
a positive childbirth experience include self-esteem, efficient and enhanced
maternal attachment and compliance [9].
Research has demonstrated that a positive childbirth
experience helps a woman develop a positive attitude towards motherhood, which
helps facilitate transition into the maternal role [10]. The positive
experience can also establish rich and successful family relations, encourage
self-esteem, improve self-confidence and ensure positive development of the
woman [11].
We need to accept that labour is a time for unique sensitivity
to environmental factors. Events and the interactions occurring during labour
have powerful psychological effects, therefore for the benefit of both the
parturient woman and her child, a positive childbirth experience is desirable
[9]. Studies also confirmed that the intrapartal nurse would be the deciding
factor on whether the woman has a positive or negative experience during
childbirth [5]. Postpartum women experience physical discomfort and
psychological changes following delivery of their infants [3].
Several scientific studies have been carried out on postpartum
care and it was found that parents valued the postpartum information they were
taught [7]; also, mothers' satisfaction with postpartum care is dependent on
their perceptions of the nurse's ability to place them at ease [11]. Nursing
care qualities that contributed to the satisfactory experience include
information sharing, calmness, demonstration of confidence and the anticipation
of unstated needs [4]. These findings illustrated qualitative inquiry for
understanding patient satisfaction with care.
The 2009 birth rate estimate in Cameroon, stood out at
31.4/1000 persons [12]. Latest survey indicated that 62% of such childbirths
were assisted by a skilled birth
attendant [13]. This indicates that health practitioners are
receiving more than half of the total births and hence a need for improved
quality of nursing care.
It is known that nursing and midwifery services are the
backbone of the healthcare system in almost all countries in the world [14].
They represent between 60-70% of the health personnel [15]. It is thus
important that we assess quality of nursing care we offer in order to improve
on it. Patient satisfaction is an important indicator.
For many years, nurses have dictated what is «good»
for their patients and how much of it is «good» because the patient
is usually entitled to receiving care. To evaluate and improve the quality of
care provided, it is of vital importance to investigate the quality of care in
the context of healthcare. Patient satisfaction is a significant indicator of
the quality of care [5].
1.2. PROBLEM STATEMENT
During the natural course of childbirth, a woman's functional
ability is limited and she is unable to control her body's natural physiologic
process. The intrapartum and postpartum patients thus rely on the clinical
assistance of the nurses and the clinical staff [16].
It is generally said that the primary reason why patients are
admitted to the health facility is to receive care that cannot be gotten
elsewhere. The major role of the nurse is to care. In our society and in most
hospitals, nurses focus on other tasks leaving out the great aspect of care.
This is revealed in their attitude towards patients, co-workers and even in the
performance of their tasks.
Although special care needs to be given to the woman during
and after the delivery periods, with the available resources manpower and time,
nurses rather tend to give patients the care they deem worth giving and not
necessarily what is required of them to meet the patients' needs. Sub-standard
care is bound to be offered. More often than not, the patients' needs are not
fully met and this makes some patients not to perceive the care as positive.
1.3. OBJECTIVES OF THE STUDY 1.3.1. General
Objectives
To evaluate the quality of nursing care offered during
intrapartum and postpartum periods using patients' satisfaction as an
indicator.
1.3.2. Specific Objectives
· Evaluate nursing care offered during intrapartum and
postpartum periods.
· Assess patient satisfaction with care.
· Identify ways of improving satisfaction hence quality of
care.
1.4. RESEARCH QUESTIONS
The following questions were drawn up to respond to the
objectives of the study.
? What nursing care is being offered during intrapartum and
postpartum periods? ? How satisfied are the patients with the care they
receive?
? How can patient satisfaction with care be improved?
1.5. HYPOTHESIS
Patients receiving intrapartum and postpartum care in BRHA are
not satisfied with the nursing care they receive.
1.6. PURPOSE OF STUDY
This study is important in measuring and improving the quality of
nursing care offered in the maternity service of BRHA. It is anticipated that
the findings in this study will aid in:
1. Identifying the quality of nursing care offered during
intrapartum and postpartum periods in BRHA.
2. Assessing patient satisfaction with nursing care.
3. Making recommendations on how patient satisfaction can be
improved.
1.7. JUSTIFICATION
Numerous study findings indicate that nursing care is the key
determinant of patient satisfaction [7]. To improve on the quality of care
provided, it is of vital importance to evaluate the care.
Intrapartum and postpartum periods are delicate periods in the
life of every woman. It is thus important that optimum care be given to the
woman during this period without which complications may arise [17].
Nurses will never know the quality of care they offer until it
is being assessed. This study on patient satisfaction, therefore, will provide
a means of evaluating the care and will provide a spring board for its
improvement.
1.8. LIMITATIONS OF THE STUDY
A number of factors limited the scope of this research
project:
A) FINANCIAL DIFFICULTIES.
The lack of financial resources was a great problem, thus making
it difficult to get enough information and carry out the research with ease.
B) TIME CONSTRAIN.
Time was also a problem the research had to take place
simultaneously with other academic work.
C) INABILITY TO PROVIDE ADEQUATE PRIVACY.
The researcher was unable to provide adequate privacy when the
patients were responding to questions. This made it more difficult since some
of the responses were influenced by the presence of other patients.
Nonetheless, this study is a necessary preliminary step toward a
better patient satisfaction with nursing care not only for those in labour but
for all will-be mothers.
1.9. OPERATIONAL DEFINITION OF TERMS
PATIENT: A person receiving medical care.
SATISFACTION: A pleasant feeling which you get
when you receive something you wanted or when you have done something you
wanted to do.
NURSING: The art and science of assisting an
individual, sick or well, by performing
those activities contributing to his/her recovery (or even to
a peaceful death), that he/she will perform unaided if he/she had the necessary
strength, will or knowledge to do this, in such a way as to gain independence
as soon as possible.
CARE: The process of protecting and looking
after someone
INTRAPARTUM: The period during labour and
delivery
POSTPARTUM: The period following the delivery of
the baby to approximately 6 weeks after delivery.
LITERATURE REVIEW
2.0. AN OVERVIEW OF LABOUR, DELIVERY AND
POSTPARTUM
A. Introduction
The physiological transition from being a pregnant woman to
becoming a mother means an enormous change for each woman both physically and
psychologically. It is time when every system in the body is affected and the
experience, though unfortunately not joyous for all, represents a major
occurrence in the woman's life [17].
According to the American Academy of Pediatrics (AAP) and the
American College of Obstetricians and Gynecologists (ACOG), labour is a
sequence of uterine contractions that results in effacement and dilatation of
the cervix and voluntary bearing-down efforts leading to the expulsion per
vagina of the products of conception. Delivery is the mode of expulsion of the
foetus and placenta [18].
The puerperium, or postpartum period, generally lasting 6-12
weeks is the period of adjustment after delivery when the anatomic and
physiologic changes of pregnancy are reversed, and the body returns to the
normal non-pregnant state [19].
B. Normal Labour and Delivery
B.1. Physiologic Preparation for Labour [20]
Prior to the onset of true labour, several preparatory
physiologic changes commonly occur:
The settling of the foetal head into the brim of the pelvis,
known as lightening, usually occurs 2 or more weeks before the onset of labour
in first pregnancies.
Braxton Hicks contractions, which are irregular, painless
uterine contractions occurring with slowly increasing frequency, during the
last 4-8 weeks of pregnancy. They are distinguished from true labour
contractions by lack of cervical change in response to such contractions.
Several weeks before the onset of true labor, the cervix
begins to soften, efface, and dilate (1-2cm), the mucus plug within the
cervical canal may be released as small amount of blood-tinged mucus from the
vagina known as bloody show.
B.2. Characteristics of True Labour [21]
These signs are usually indicative that true labour has begun:
1. Regular painful uterine contractions occurring frequently
about 3-6 times in every 10-20 minutes.
2. Dilatation of the cervical os.
B.3. Physiology of Normal Labour [22]
Normal labour is a continuous process that has been traditionally
divided into three stages for purposes of study: the first, second and third
stages.
· The first stage of labour, further subdivided into the
latent, active and transitional phases, is the interval between the onset of
labour and full cervical dilatation.
· The second stage is the interval between full cervical
dilatation and delivery of the baby.
· The third stage of labour is the period between the
delivery of the baby and the delivery of the placenta.
B.3.1. First Stage of Labour:
The duration of the first stage of labour in primiparous
patients is noted to range from 6-18 hours, while in multiparous patients the
range is reported to be 2-10 hours. The lower limit of the normal for the rate
of cervical dilatation during the active phase is 1.2 cm per hour in first
pregnancies and 1.5 cm per hour in subsequent pregnancies.
The latent phase is prior to the active phase and last 6-8
hours. The cervix dilates from 0 to 3-4cm. The length of the cervix shortens
from 3cm to less than 0.5cm long.
The active phase begins when the cervix is about 4cm dilated and
ends at full dilatation (10cm).
The Transitional phase is from 8cm dilation until expulsive
contractions are felt by the woman.
B.3.2. Second Stage of Labour:
The second stage generally takes from 30 minutes to 3 hours
in primigravid women and from 5-30 minutes in multigravid women. The median
duration is 50 minutes in primipara and 20 minutes in multipara.
The transition period between the first and second stage is
marked by more frequent contractions and often server pain. Symptoms are
increased in bloody show and a feeling of pressure on the rectum accompanied by
a desire to bear down with each contraction. The descent of the fetus also
called the station, is evaluated to assess the progress of labour. It is done
by measuring the relationship of the bony portion of the foetal head with
respect to the maternal ischial spines. According to ACOG, when the bony
portion of the foetal head is at the level of the ischial spines, the station
is 11011.
The mechanism of labour in the vertex position consists of
engagement of the presenting part, flexion, descent, internal rotation,
extension, external rotation, and expulsion of the baby in this chronological
order.
B.3.3. Third Stage of Labour:
This is the stage of separation and expulsion of the placenta
and its membranes. It usually last for 2 hours in primigravids and 1 hour for
multigravids. Separation of the placenta generally occurs within 2-10 minutes
by the end of the second stage, but it may take 30 minutes or more to
spontaneously separate.
Signs of placental separation are:
v' A fresh gush of blood from the vagina.
v' The umbilical cord lengthens outside the vagina.
v' The fundus of the uterus rises up.
v' The uterus becomes firm and globular.
When these signs appear, it is safe to place traction on the
cord. The gentle traction, with or without counter-pressure between the
symphysis and fundus to prevent descent of the uterus, allows delivery of the
placenta.
C. The Postpartum Period (Puerperium)[23]
The puerperium consists of the period following the delivery of
the baby and placenta to approximately 6 weeks postpartum and further
classified as:
- Immediate Postpartum 4 Birth to 24 hours
- Early Postpartum 4 24 hours to 1 week
- Late Postpartum 4 1 week to weeks
The immediate postpartum period is a critical time for both
maternal and neonatal physiologic and emotional adjustment. It is during this
time that most postpartum complications occur.
C.1. Different phases of postpartum [17]
The postpartum period has three phases:
· «Taking in» phase:
During the taking in phase, which is within the first 24 hours after delivery,
physical recovery occurs. The mother is passive and dependent needing to be
mothered herself. She is fatigued after the hard work of labour and needs
nourishment, rest and sleep. However, she also needs her baby so that the
attachment phase can continue.
· Following the taking in phase, the woman goes through
the «taking hold» and «letting go»
phases. It has generally been accepted that these phases last 3 to 14
days each. In the «taking hold» phase, the woman gains control over
her body and assume her independence and autonomy. In the letting go phase, the
woman establishes new maternal role patterns.
C.2. Postpartal Systemmic Adaptations
A comprehensive nursing assessment is based on a sound
understanding of the normal physiologic process of puerperium:
C.2.1. Uterine Changes
1. Uterine Involution.
The uterus increases markedly in size and weight during
pregnancy (about 10 times the non-pregnant weight, reaching a crude weight of
about 1000 g) but involutes rapidly after delivery to the non-pregnant weight
of about 50 to 100 g at an average rate of 1cm/day.
Patient Satisfaction with Intrapartum and Postpartum Nursing
Care: Buea Regional Hospital Annex.
Immediately following delivery, the uterus weighs about 1 kg,
and its size approximates that of a 20-week pregnancy (at the level of the
umbilicus). At the end of the first postpartum week, it normally will have
decreased to the size of a 12-week gestation and is just palpable at the pubic
symphysis. During involution, the size of the cells decrease markedly but there
is no decrease in number. The outermost layer becomes necrotizing and is
sloughed off in lochia. Proteolytic enzymes promote autolysis except at the
placenta site [24]. Involution usually causes myometrial contractions or after
pains and last three weeks. Breastfeeding increases such contractions due to
further release of oxytocin. Mothers might need a first class analgesic.
2. Changes in fundal position.
Following expulsion of the placenta, the uterus contracts
firmly to the size of a large grape fruit. Walls of the uterus are about 4 to 5
cm in diameter. After birth, the top of the fundus remains at the umbilicus for
about half a day. On the first day following birth, the fundus is 1cm below the
umbilicus. The top of the fundus descends 1cm or a finger breath per day until
it descends into the pelvis about the tenth day [17].
3. Lochia .
One of the unique capabilities of the uterus is its ability to
rid itself of the debris and remains after delivery. This discharge, termed
lochia is classified according to its appearance and content:
v' Lochia rubra is dark red in color persisting for
2-3 days and contains erythrocytes,
epithelia cells, leukocytes, bacteria,
lanugo and occasionally fetal meconium [10].
v' Lochia serosa is pinkish to brownish. It flows
from about the 3rd day to 10th day composed of serous
exudates shreds of decidual erythrocytes, leukocytes, cervical mucus and
numerous micro-organisms.
v' Lochia Alba is composed of primary leukocytes,
decidual cells, epithelia cells, fat cervical mucus, cholesterol crystals and
bacteria [10].
Lochia has a stale musty odour which is not offensive.
4. Cervical changes.
Following birth, the cervix is spongy, flabby and formless.
It appears bruised but the original form of the cervix is regained within a few
hours. The cervical os admits two fingers for a few days following birth but
only one finger by the end of the first week. Change of shape of the os is
permanently changed by child bearing [24].
5. Uterine Vessels
Successful pregnancy requires a massive increase in uterine
blood flow. To provide for this, arteries and veins within the uterus, and
especially those of the placental site, enlarge remarkably, as they transport
blood to and from the uterus. Within the uterus, growth of new vessels also
provides for the marked increase in blood flow. After delivery, the caliber of
extra uterine vessels decreases to equal, or at least closely approximates that
of the pre pregnant state. Within the puerperal uterus, larger blood vessels
are obliterated by hyaline changes which are gradually resorbed, and replaced
by smaller ones.
C.2.2. Vaginal and Perineal Changes
Following birth, the vagina appears oedematous and may be
bruised. Lacerations may be present and rugae obliterated. The site of vagina
decreases and rugae returns to normal within 3 weeks. Soft tissue in and around
the perineum may appear oedematous with some bruising.
C.2.3. Mammary glands
After birth, the inter play of maternal hormones leads to the
establishment of milk production at the level of the mammary glands of the
breasts. This occurs through a series of mammogenesis (cellular multiplication
at the start of pregnancy) and lactogenesis (cellular differentiation by the
end of pregnancy).
Rapidly increasing Progesterone levels causes secretion of
prolactin, which in turn causes milk letdown to be effective within the first
(24-48) hours after delivery. Such breasts are usually swollen, tender and
febrile on touch.
Colostrum flows for about 5 days, which gradually becomes
converted to full milk by the 4th week.
C.2.4. Weight Loss
In addition to the loss of about 5 to 6 kg due to uterine
evacuation and normal blood loss, there is usually a further decrease of 2 to 3
kg through diuresis. Most women approach
their self-reported pre-pregnancy weight 6 months after delivery
but retain an average surplus of 1.4 kg
C.2.5. Urinary System
The postpartal woman has an increased bladder capacity,
swelling and bruising of the tissue around the urethra, decreased sensitivity
to fluid pressure hence at risk of over distention and incomplete emptying.
Urinary output increases during early postpartum due to puerperal diuresis
[25].
C.2.6. Gastro-Intestinal System
Hunger following birth is common and the mother may enjoy a
light meal. Frequently, she is thirsty and will drink large amounts of fluid.
Bowels tend to be sluggish after birth because of the lingering effects of
progesterone and decrease abdominal muscle tone [17].
C.2.7. Changes in Vital signs
During the postpartum period, with the exception of the first
24 hours, the woman should be afebrile. Blood pressure should remain stable and
within normal range following birth. Puerperal bradycardia with rates of 50 to
70 beats per minute commonly occurs during the first 6 to 10 days [26].
C.2.8. Others
Temporal amenorrhoea within 6-12 weeks in 100% of
non-breastfeeding mothers, and about 36 weeks in 70% of mothers carrying out
effective breastfeeding.
Ovulation occurs only after 40 days for non-breastfeeding
mothers and may extend right up to 6 months for breastfeeding mothers due to
the inhibitory effect of prolactin on FSH through a negative feedback
mechanism.
Hypercoagulability due to triggering of the intrinsic pathway
by thromboplastin, massively released in the course of placental detachment.
This poses a high risk of thromboembolic complications within the first 3 weeks
following delivery.
C.3. Postpartal Psychological Adaptations
C.3.1. Depression
It is common for a mother to exhibit some degree of depressed
mood a few days after delivery. This situation, termed postpartum blues,
describes a transient period of
depression that occurs in most women during the first week or
two after birth. It is manifested by mood swing, anger, weepiness, anorexia,
difficulty sleeping and a feeling of letting down. It is likely the consequence
of a number of factors:
v' The emotional letdown that follows the excitement and fears
that most women experience during pregnancy and delivery.
v' The discomforts of the early puerperium.
v' Fatigue from loss of sleep during labour and postpartum.
v' Anxiety over her capabilities for caring for her infant after
leaving the hospital. v' Fears that she has become less
attractive.
In the great majority of cases, effective treatment need be
nothing more than anticipation, recognition, and reassurance. This mild
disorder is self-limited and usually remits after 2 to 3 days, although it
sometimes persists for up to 10 days. Should postpartum blues persist or
worsen, a careful search should begin for symptoms of major depression, which
can occur in almost 20 percent of puerperal women [24].
C.3.2. Maternal Role
During the first two days, the woman turns to be positive and
somewhat dependent. Maternal role attainment therefore is a state whereby the
woman learns about her behavior and becomes comfortable with her identity as a
mother [17].
Although post partum period is a time of many physiological
and psychological changes, the stressors, they are usually considered good and
are not unhealthy [27].
C.3. Postpartum Complications
Several factors can hinder the normal physiological and
psychological puerperal evolution. Such complications greatly account for the
geometrically increasing maternal mortality in a developing country like
Cameroon from:
v' 430 deaths/100.000 in 1990
v' 669 deaths /100.000 in 2000
1' 1000 deaths/100.000 in 2010 [EDS 2010
(national statistics and demographic data)] Maternal
mortality according to WHO is the death of a woman when she is pregnant, in
labour or within the 42 days following termination of the pregnancy due to
obstetrical induced causes [28]. These values are relatively quite explosive,
with a woman dying each minute due to pregnancy complications [29].
These postpartum complications are:
1. Postpartum Haemorrhage: This is the leading
cause of maternal mortality (24.8%) and noticed in 5% of total pregnancies
worldwide [30]. It is defined as excessive bleeding greater or equal to 500ml
following a per vagina delivery. It is termed «severe» if values
exceed 1000ml. Possible aetiologies include:
v' Persisting uterine atony (70-90)%.
v' Obstetrical genital lacerations (cervical, vaginal and
perineal tears).
v' Retention of placental debris.
v' Others (retention of the entire placenta, haemorrhagic
endometritis, uterine inversion, uterine rupture, coagulopathies such as
DIVC).
2. Infection: Second leading cause of maternal
mortality after bleeding
(14.9%) [30]. The most common infectious causes of puerperal
fever include:
v' Endometritis usually due to premature rupture of
membranes.
v' Urinary infections (pyelonephritis).
v' Breast pathologies (lymphangitis, galactophoritis).
3. Pre-eclampsia / Eclampsia: Third major cause
of maternal mortality
worldwide (12.9)% and 25% of all eclampsia occurs during
postpartum[30]. Pre-eclampsia is a diastolic blood pressure greater or equal to
90mmHg measured 4hours apart (or 110mmHg in a unique measurement) associated
with a proteinuria of (0.3-5) g/l within 24 hours and occurring at a
gestational age at 20 weeks and above. Eclampsia is simply pre-eclampsia
associated with tonico-clonic convulsions [31].
4. Thrombo-embolic diseases: Usually are caused
by hypercoagulability.
Favourable factors include age (above 40 years), multiparty,
obesity,
dystocia or difficult labour, underlying cardiac pathologies
and past history of thromboembolic diseases. The most common manifestations are
pelvic phlebitis, superficial and deep venous thrombosis.
5. Anemia: Usually occurs following hemorrhage.
However, could also be Pre-existent. Characterized clinically by
cutaneous-mucosal pallor of the conjunctivae, gums, tongue, palates, palms of
the hands and soles of the feet. Biologically, it is a hemoglobin level less
than or equal to 10 g/dL in pregnancy.
Patient Satisfaction with Intrapartum and Postpartum Nursing
Care: Buea Regional Hospital Annex.
6. Puerperal Psychosis: Psychic disorders
usually during the late postpartum. About (1- 2)/1000 women who deliver suffer
from postpartum blues which when severe can lead to delirium, mania, depression
and other schizophrenic states [10]. Suicidal thoughts are not uncommon.
7. Puerperal Neuropathiess Characterised by
nervralgia, cramps and
Sometimes paralysis of the femoral and obturator nerves.
8. Spontaneous Symphysiotmy: This refers to
a disjunction of the pelvic bones at the pubic symphysis following delivery.
Clinically it is painful and normal function is impaired. On an x-ray, there is
a lateral luxation of the pubic symphysis as shown below.
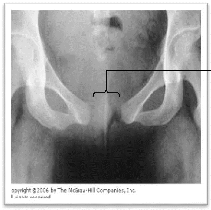
Figure 1:
An abdomino-pelvic x-ray (front view), showing a disjunction of
the pelvic bones following a
Lateral luxation
2.1. NURSING CARE AND RESPONSIBILITIES
A. Introduction
The unique function of a nurse is to assist an individual,
sick or well, by performing those activities contributing to his/her recovery
(or even to a peaceful death), that he/she will perform unaided if he/she had
the necessary strength, will or knowledge to do this, in such a way as to gain
independence as soon as possible [26].
In general obstetric nursing care, the objectives are aimed
at reducing maternal and neonatal mortality through a careful follow-up during
labour and delivery, as well as prevention and management of eventual
complications during the postpartum period
Therefore understanding the role of nursing care during these
periods is integral.
B. Nursing role during labour and delivery
The goal of nursing care during the birth process is to
instill maximum physical and emotional wellbeing of both the woman and the
foetus. This goal includes the transition of woman to mother and foetus to baby
[32].
To implement proper care, the nurse must be familiar with
normal physiology of labour, deviations from the norms and adjustments,
self-confidence and skill required to cope with the stressful and emergency
conditions. However, knowledge and technical ability are not sufficient in
themselves the nurses must also address the psychological aspect of care by
conveying warmth and empathy [33].
B.1.) On Admission
First impressions are vivid [26]. Parturients and their partners
need to feel welcomed.
· The nurse greets them in a calm and pleasant manner.
· The patient is taken into the labour ward for assessment
and evaluation, together with her belongings (delivery accessories, baby's
wears)
· The nurse helps the patient undress and gets into
hospital gown.
· The patient is made comfortable and may lie in the left
lateral decubital position.
· The labour ward needs to be tidy, well lit and airy
enough to accommodate patient and
her husband. Room kept at comfortable
temperature levels between (37.8 - 40) oC.
· A warm blanket placed over the patient and one wrapped
around her feet are very comforting.
· The nurse then develops a rapport and establishes the
nursing database, comprising of a concise patient obstetrical and medical
history.
· After obtaining essential information from the patient,
the nurse may then begin intrapartal assessment and evaluation [32].
B.2.) Intrapartum Clinical Assessment and
Evaluation
B.2.1. Nursing Management of First Stage of Labour
[33]
· First the vital signs are taken and noted. These
include: temperature, blood pressure, pulse rate, respiratory rate. At this
time, the foetal heart tones are auscultated using a foetoscope (normal foetal
heartbeats of (140-160)/min.)
· Anthropometric measurements are equally taken and
noted. These are: corporal weight, height, abdominal girth, fundal height (FH)
from which the estimated foetal weight (EFW) can be derived using Steven
Johnson's formula [35]:
Figure 2: Estimated Foetal Weight
EFW = I 155 x (FH - n) + 275
]g
|
|
Where :
n = 12 if head is not engaged n = 11 if head is
engaged
FH = Fundal height
EFW = Estimated Foetal Weight (normal) = (2.500 -
3.800)g
|
|
· A clean-voided midstream of urine specimen is collected
and a dipstick test rapidly conducted for proteins, ketones and glucose
[25].
· Number of uterine contractions is noted every after 10
minutes while simultaneously appreciating the intensity and duration of each
contraction. In specialized centres a cardio-tocogram is preferable used to
monitor the effects of such contractions on the
foetal heartbeats. This is an essential element in the
assessment of materno-foetal wellbeing.
· Aseptic vaginal exams are done after every 2 hours using
a pair of sterile gloves and an antiseptic solution to assess the cervix, the
presenting part and the membranes.
· At a cervical dilatation of 4cm, 2-4 regular
contraction in 10 minutes each lasting 40-60 seconds; a partogram should be
opened. This vital tool is of imperative significance as it effectively detects
dystocic labour (obstruction and cephalo-pelvic disproportion) as well as acute
foetal distress. It also sets landmarks (the alert and action lines) where an
intervention must be carried out to guarantee materno-foetal wellbeing. Such
interventions could be induction of labour mechanically or pharmacologically,
augmentation of labour, assisted delivery by forceps or vacuum extractor, an
emergency cesarean section [33].
· Cervical assessment is better evaluated using the Bishop
Scoring system as shown below: [35]
Table 1: The Bishop Scoring System
SCORE
FACTOR
|
0
|
1
|
2
|
3
|
Dilatation (cm)
|
0
|
1 - 2
|
3 - 4
|
> 5
|
Effacement (%)
|
30
|
40 - 50
|
60 - 70
|
> 80
|
Station
|
-3
|
-2, -1
|
0
|
+1, +2
|
Cervical Consistency
|
firm
|
medium
|
soft
|
|
Cervical Position
|
posterior
|
median
|
anterior
|
|
|
· A bishop score <7/13 requires that labour should be
stimulated using mechanical or pharmacological methods.
· If patient has not had child education classes, the
latent phase is time when the nurse can have anticipation guidance, teaching on
breathing techniques to cope with such contractions. Breathing techniques can
promote relaxation of abdominal muscles and
Patient Satisfaction with Intrapartum and Postpartum Nursing
Care: Buea Regional Hospital Annex.
increase size of the abdominal cavity lessening discomfort
during contraction of uterine wall.
· Dietary intake must be limited to sips of clear fluids
and ice chips at frequent intervals. Cleaning of the mouth with toothbrush or
glycerin swabs help to counteract the dry and thirsty sensations of the
mouth.
· IV fluids may be ordered to counteract dehydration and
provide energy. An infusion of 500ml of 5% Dextrose, or 500ml of Hartman's
solution depending on the indication is administered to keep veins open.
· Analgesia may be administered during a
well-established contraction if the patient is not to give birth within the
next 1 to 2 hours. If analgesia is administered the patient must remain in bed
for safety [24].
· The patient is advised to void at least every 2hours.
If patient is not on IV medications, or the presenting foetal part not engaged
or membranes not ruptured, she has bathroom privileges otherwise she uses a
bedpan. A foley's urinary catheter may be used in case of inability to void
[45].
· Showers or bed baths may be taken depending on progress
of labour. Allowing warm water to strike lower part of the back may be very
relaxing
· A cleansing enema may be ordered on admission because
some women experience loose stools prior to active labour.
· If the amniotic membranes have not ruptured
previously, they may be ruptured artificially as a mechanical means of inducing
labour. The time of rupture, colour and odour of the amniotic fluid is taken
and noted. Note that this is accompanied by a continuous monitoring of
predicting parameters of maternal and foetal wellbeing [25].
B.2.2 Nursing Management of Second Stage of Labour
[31]
· Nurse provides comfort and support during the
patient's pushing effort and encourages her to push harder and not let any
breath out or to put all her effort into the push and not into making noise.
· When the patient feels an uncontrollable urge to push
(bear down), the nurse can help by encouraging her positioning.
· Most patients respond positively to touch in labour.
They appreciate deft, gentle handling by the staff. The patient's awareness of
the soothing qualities to touch changes the labour process and many patients
develop hyperesthesia during labour.
· Breathing techniques are used to increase abdominal
pressure thus assisting in expelling the foetus.
· It is important to note that tension and fear are part
of the cycle of pain and everything possible should be done to reduce it. This
includes giving information both before and during labour .
· Constant presence is vital. Words of praise, comfort,
encouragement and reassurance will vary from nurse to nurse [35].
· Mobility and positions for labour: The freedom to move
and adopt different positions is an important way of helping women to cope with
the pain of labour and may aid progress [35].
· Distraction is another means of increasing relaxation and
coping with discomfort. During early labour, light cards or other games may
serve as distraction.
· Time of birth is noted. Baby's birth weight, cranial
perimeter, brachial and thoracic perimeters, and the APGAR score are noted.
· Immediately after birth, the care given focuses on
assessing and stabilizing the newborn. As the head is being delivered,
suctioning of the baby is done. Moist gauze sponges are used to wipe the nose
and the mouth.
· Where the baby is placed should be warm, hygienic,
vitamin K is administered for hemostasis. Gentamycine eye drops given as
prophylaxis against neonatal conjunctivitis. The clamped umbilical cord is
cleaned with alcohol and covered with sterile gauze.
· Brief assessment of the baby can be performed when the
mother is holding the baby. This includes checking baby's airway.
· Baby should be dressed in the appropriate baby's wears as
fast as possible to minimize hypothermia.
· To ensure correct identification the nurse gives the
mother matching identification bands in the delivery room.
·
To enhance attachment, breastfeeding can be encouraged if the
mother and the baby desire.
· While waiting for signs of placental separation, the
nurse gently palpates the uterus to check for ballooning caused by uterine
relaxation and subsequent bleeding into the uterine cavity [22].
B.2.3. Nursing Management of Third Stage of Labour
[25]
This process is an active one due to the high risk of
haemorrhage involved. It is therefore usually referred to as Active Management
of Third Stage of Labour (AMTSL) divided into 7 well-defined stages.
1. Firstly immediately after expulsion of the baby, verify
absence of a second foetus by palpating the abdomen.
2.
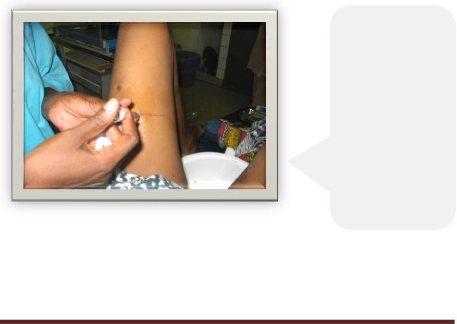
Figure 3:
Active Management of third satge of labour.
A patient here is being injected intra-muscularly with 4ml of 10
I.U. Syntocinon.
Secondly, administer 10 IU of Oxytocin intramuscularly as shown
below.

Figure 5: Examination of the placenta.
This midwife is inspecting the shiny amnion making sure it is
intact.
3. Thirdly, wrap the maternal umbilical cord around the clamp and
wait for the next uterine contractions as shown below:
4.

Delivering the placenta by continuous traction on the umbilical
cord.
Figure 4:
Exercise continuous traction on the umbilical cord
45o below the horizontal to prevent detachment from the placenta,
meanwhile also continue applying a counter pressure against the uterus pushing
it upwards and 45o above the horizontal.
5. After delivery of the placenta, massage the uterus.
6. Examine the placenta, as shown below:
In examining the placenta, check both the maternal and foetal
faces. In the maternal face: - Look out for calcifications whether there are
blood clots, fibrosis etc.
- Inspect the membranes for missing portions.
- Examine the cotyledons (16-18 irregular lobes of connective
tissue separated by septa formed during placentogenesis) .
In the foetal face:
- Check if the shining amnion is intact.
- Inspect the blood vessels embedded in the chorion
- Carefully check for proper insertion of the umbilical cord.
· Finally weigh the placenta, which is usually
1/6th the weight of the foetus ( 500g). The Nurse disposes of the
placenta according to the wish of the mother. Women usually carry it home and
dispose of it according to their custom [25].
· Lacerations are repaired or episiotomies sutured. The
vulva area is gently cleansed
with warm sterile water or normal saline and
sterile pads applied to the perineum.
· The nurse should record the following information
about the delivery of the placenta. Exact time, whether it was delivered
spontaneously, which side of the placenta presents.
· Examination of cervix, perineum cleaned, woman's gown
changed and woman placed comfortably to rest.
· Following the delivery, the woman might feel chilled and
shake uncontrollably. She should be covered with a warm blanket to provide
warmth.
· Nurse should note reaction of the mother and help her to
adjust.
C. Nursing role during the postpartum period
After delivery, both the mother and the baby will have health
concerns that need to be addressed attentively. Although pregnancy is
considered to be wellness oriented, the nurse needs critical thinking skills to
provide safe, high quality nursing care [31].
C.1. Immediate postpartum care [23]
The first four hours after delivery is a critical period.
Postpartum haemorrhage is most likely to occur. Thus the following should be
done [25].
1. Check blood pressure every 15 minutes for 1-2 hours until it
is stable, then every 4- 12hours.
2. Check uterine fundus, lochia and episiotomy alongside vital
signs.
3. Check signs of haemorrhage.
4. Monitor for bladder distention and record first voiding.
5. Monitor interaction with infant. If signs of bonding are not
present, determine possible aetiology: pain, complication, or psychological
instability.
6. Relieve discomfort in an oedematous perineum, distended
bladder, perineal lacerations, vaginal haematoma, and engorged breasts.
7. Avoid leaving patient alone.
C.2. Subsequent Care [31]
· Provide a quiet and comfortable environment for the
mother.
· Check breast, fundus, lochia, stitches if present,
bladder, bowels and legs at least once every shift .
C.2.1. Perineal care.
· Teach patient perineal care using a Sitz bath .
· Teach patient how to use perineal pads, anaesthetic
sprays or ointments for relief of pain.
· Teach patient how to contract her buttocks when sitting
to prevent complications [26]. C.2.2. Voiding
· Check voiding patterns if patient's urethra or bladder is
traumatized may be by a fistula, catheterization should be done.
· Teach patient how to void every several hours to keep her
bladder empty. C.3. Breast care .
· Assess conditions of patient's breast and nipples for
redness, ulcerations and firmness.
· Teach patient how to wash her breasts and nipples with
warm water and avoid removing the protective skin oil.
· Teach patient how to wear brassieres or breast binders
that provide good support day and night .
· Lactation suppressants may be given to non-breastfeeding
mothers.
· Check breasts for signs of engorgement, (swollen,
tender, shiny breast tissue) for engorged breasts, use hot compress to improve
comfort, express some milk, a mild analgesic to improve comfort.
· Teach patient ideal positioning for breastfeeding.
· Teach patient the importance of breastfeeding, making
sure she knows the advantages of effective breastfeeding:
v' It is costless in monetary terms.
v' It is always available.
v' It is rich in immunoglobulins A and hence prevents
infections.
v' It contains nutrients in their correct proportions.
v' It is being stored under ideal temperatures.
C.4. Care of baby.
Complete clinical examination of the mother is important in
order to know her state.
C.5. Newborn care.
· A newborn physical assessment is done at least three
times within the first 12 hours of life.
· Verify notification of baby.
· Thermoregulation may be maintained by skin to skin
contact, using a warm blanket and radiant warmer.
· Teach mother about infant stimulation techniques, signs
and symptoms in the infant that indicate possible problems, baby's bath and
cord care [25].
· The mother's wellbeing is inter-dependent with that of
her baby as they adjust to
multiple physical cognitive and psychosocial
changes during the puerperium period.
2.2. PATIENT'S PERCEPTION OF NURSING CARE (PATIENT
SATISFACTION)
There exist scientific ways of measuring health care quality
[34].
These tools have mostly been used by health professionals to
review and improve the quality of care they provide.
A reliable indicator is by means of information gotten from
the patients or an operational process that is converted into a rate,
percentage or time that shows how well providers are taking care of their
patients. Quality measures give information about how well providers care for
some but not all of their patients. Quality care enhances patient's
satisfaction and their use of services.
It is known that the nursing profession has only recently
began to look at what the term caring really means [5]. In current care
environments, the measurement of patients satisfaction defined by some
investigators as patient's perception of quality of care has become important
as hospitals compete for patients and struggle to control cost.
Nursing care has been found to be the most important variable
influencing overall patient satisfaction. Caring is now viewed as a central
component of nursing intervention necessary for cure to take place, the moral
and ethical basis of nursing and the essence of nursing [26].
Majority of studies shows that nurses place more emphasis on
task dimensions than the affective dimensions. Patients value the affective
dimension and want nurses to be kind, friendly, considerate, careful and gentle
as well as provide proficient and timely technical skills [33]. Several patient
characteristics influence perception of care: age, gender and degree of pain.
Male patients focus on physical aspects of care and female patient focus on
emotional aspects. Patients in pain need more care [5].
The determination of nursing care effectiveness in improving
client outcomes is accompanied through outcome measures [26]. Health care
consumers are well able to define the quality of care they receive. The
increased emphases on quality improvement in health care agencies bring with it
the recognitions that quality is a dynamic costumer perception. Dissatisfaction
results when customer expectations are not met.
It is known that patients perceived different levels in terms
of quality of care [34]. The quality depends on certain contextual intervening
conditions pertaining to the broader environments, perception may thus be
considered from four dimensions:
v' The medical technical competence of the caregiver,
v' The physical-technical conditions of the care
organizations,
v' The degree of identity-orientation in attitudes and
v' Actions of the caregiver and the socio-cultural atmosphere
of the care organization. The nurse-patient relationship according to research
sets the tone of care experience and has a powerful impact on patient
satisfaction. The patients see how the nurses interact based on their
observations. In addition, nurses' attitudes towards their work, co-workers and
organizations affect patient and family judgment
If we want to improve quality of care we provide, we must be
able to measure the performance; nevertheless health care providers have
limited ability to obtain feedback regarding performance in their daily work
due to:
? a lack of information system and lack of agreement on how to
measure the quality of care.
v' resistance to raise service standards is understandable
when nurses perceive leaders as doing too little to remove obstacles to provide
excellent health care services. Broken equipment, linen shortages, short
staffing, inadequate support in the phase of disrespectful doctors, all of
these and more obstacles cause nurses to say «don't pin patient
satisfaction on us, we don't have enough support we need to provide the care we
want to provide» [8].
METHODOLOGY
3.1. Study design
This was a descriptive study on the outcome using both
qualitative and quantitative research methods. A cross section survey was
chosen for the study. Systematic random sampling was used for selection of the
study participants.
3.2. Study period:
This study was conducted over a period of 4 months (March to June
2009).
3.3. Study site
This study was carried out in the Fako Division of the Southwest
Region of Cameroon specifically at the Maternity unit of the Buea Regional
Hospital annex.
Figure 6: Sketch diagram of BRHA.
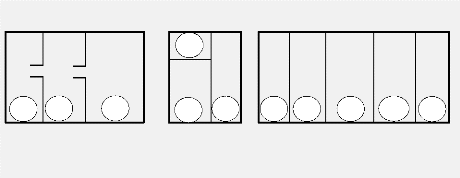
1 2 3
4
5
6
Legend
|
1.
|
Nursery
|
5.
|
Toilet and sink
|
|
2.
|
Vestry
|
6.
|
Labour room
|
|
3.
|
Nurse's station
|
7.
|
Postnatal wards
|
|
4.
|
Delivery room
|
8.
|
Bathroom and Toilet
|
The hospital has various units: the emergency unit, surgical
unit, theatre, medical unit, HIV/AIDS and Tuberculosis treatment centers, the
maternity, family planning center, the pharmacy and mortuary departments.
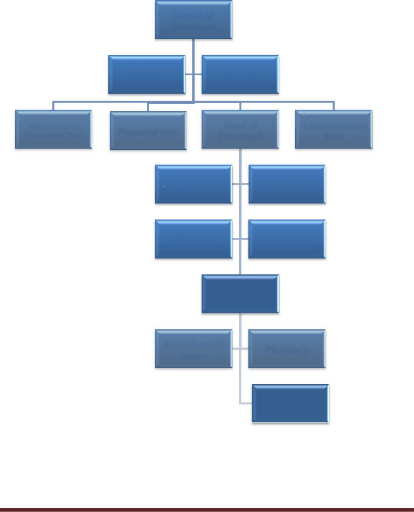
The maternity unit of this hospital was used for the study. It
is a first referral unit of choice, made up of a variety of staff : Doctors,
Nurses, and support staff. It is headed by a Head of Personnel. (see organigram
of hospital below)
Financial Unit
Pharmacy
Personnel
Head of Stores accountant Unit
Director of medical
Services Assistant
HIV/AIDS and TB
Centers
Surgical Unit Emergency Unit
Maternity Medical Unit
Board of
Directors
Family Planning
Center
Head of
Personnel
Administrative
Unit
Figure 7. Organigram of the BRHA
3.4. Study population
Women in the maternity ward who are receiving postpartum care
after delivery in the Hospital. The questionnaire was in the English language
and was self-administered. Illiterate patients had the questionnaire read and
translated to them in pidgin and the responses were indicated by the
researcher.
3.5. Sampling method
The sampling method used was systemic random sampling. Women
present in the ward who had been delivered of their babies at least one day ago
either per vagina or emergency caesarian sections were served the
questionnaire
3.5.1. Inclusion criteria
Women who put to birth per vagina or through emergency caesarian
section and had been in the ward for at least 24 hours were included in the
study.
3.5.2. Exclusion Criteria
Women who did not meet the above criteria were excluded from the
study.
3.6. Sample size
We chose a convenient sample size of 37 including all age
groups.
3.7. Data collection procedure
The main tool for data collection was a self-administered
questionnaire. Before data collection was done, a letter of authorization was
collected from the Dean of the Faculty of health sciences, University of Buea.
Questionnaires were then administered from the 23rd of April to the
12th of May 2010.
3.7.1. Validity of the instrument
The questionnaire was pretested in Mount Mary maternity. Some
questions were then modified or reformulated to adapt to the local
conditions.
3.7.2. Data Entry and Analysis
Data was entered and analyzed using Microsoft Excel 2010 and
the Statistical Package for the Social Sciences, SPSS version 14.0. Descriptive
statistics including frequency, means, percentage and standard deviation were
employed. The results were presented in tables, pie charts and bar charts.
3.8. Ethical considerations
v' Informed consent.
v' Respondents were given a verbal consent before the
questionnaires were administered to them.
v' Confidentiality and privacy
v' Respondents remain anonymous and respect given to their
privacy.
v' All information collected was kept by the researcher until
presentation.
3.9. Budget
This project took an estimated cost of 150.000 CFA francs.
PRESENTATION AND ANALYSIS
OF RESULTS
Patient Satisfaction with Intrapartum and Postpartum Nursing
Care: Buea Regional Hospital Annex.
4.0 Introduction
The results of this study have been presented per objective for
easy and logical discussion in this chapter.
4.1 Socio-Demographic Data
This involves age distribution, parity status, educational level,
marital status, profession and the number of days spent in the maternity.
Figure 8: Age Group Proportions
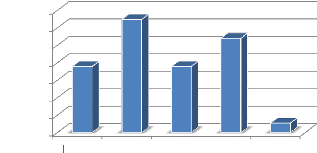
[16;20[ [20;25[ [25;30[ [30;35[ [35;37[
27.00%
2.70%
Proportions
35.00%
30.00%
25.00%
20.00%
15.00%
10.00%
5.00%
0.00%
18.90%
32.40%
18.90%
Age Groups (years)
4.1.1. Age distribution Table 2:
Distribution according to Age.
|
Age Groups (years)
|
Mean
Age (x)
|
Frequency
(f)
|
Proportion
|
f(x)
|
|
[16;20[
|
18
|
7
|
18.9%
|
126
|
|
[20;25[
|
22.5
|
12
|
32.4%
|
270
|
|
[25;30[
|
27.5
|
7
|
18.9%
|
192.5
|
|
[30;35[
|
32.5
|
10
|
27.0%
|
325
|
|
[35;37[
|
36
|
1
|
2.7%
|
36
|
|
Total
|
|
37
|
100%
|
949.5
|
The greatest proportion of the population (32.4%) is between
the age group of (20 and 25)
with a mean age of 25.7
4.1.2. Levels of Education
Table 3: Distribution according to Levels of Education.
Levels of Educations Frequency Proportions
None 1 2.9%
FSLC 16 47.1%
O/L 6 17.6%
A/L 4 11.8%
1st Degree 5 14.7%
DIPES I 1 2.9%
CEP 1 2.9%
Total 34 100%
2.90%
47.10%
17.60%
14.70%
11.80%
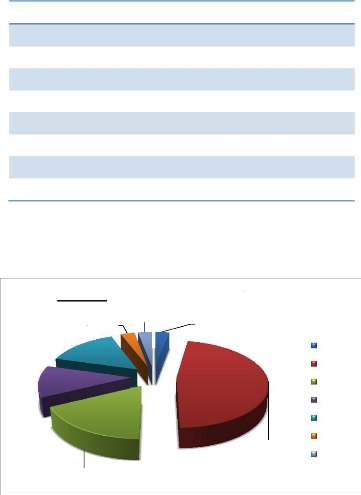
Figure 9: Proportions by Level of
Education
2.90% 2.90%
None FSLC O/L A/L
DEGREE DIPES I CEP
Majority (47.1%) of the population were FSLC holders.
4.1.3. Professional Distribution
Table 4: Distribution according to Profession.
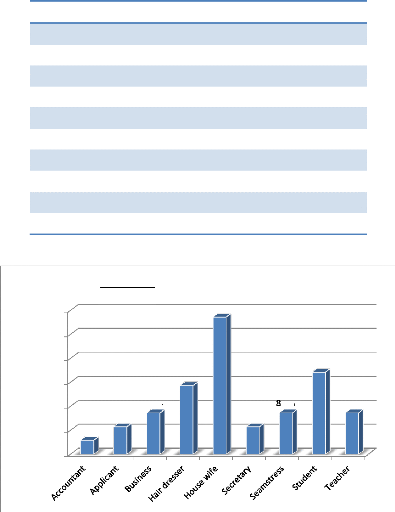
PROFESSION Frequency Proportions
Accountant 1 2.9%
Applicant 2 5.7%
Business 3 8.6%
Hair dresser 5 14.3%
House wife 10 28.6%
Secretary 2 5.7%
Seamstress 3 8.6%
Student 6 17.1%
Teacher 3 8.6%
Total 35 100%
28.6%
30.0%
25.0%
20.0%
17.1%
14.3%
15.0%
8.6%
.6%
8.6%
10.0%
5.7%
5.7%
2.9%
5.0%
0.0%
Proportions
Figure 10: Professional Distribution
Low and no income earners constituted the majority with house
wives making up 28.6% of
the total population.
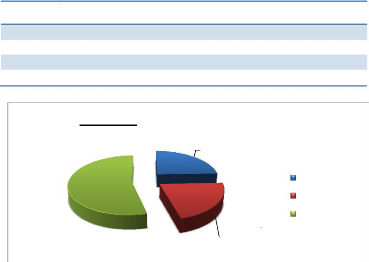
4.1.4. Marital Status Distribution
Table 5: Distribution according to Marital Status.
Marital status Frequency Proportion
Married 25 67.6%
Single 12 32.4%
Total 37 100%
Figure 11: Marital status
|
32.40%
|
|
67.60%
|
|
Married Single
|
A greater proportion of the population (67.6%) were married.
4.1.5. Number of days spent at Maternity
Table 6: Distribution according to Number of days spent at
Maternity.
Number of days Frequency Proportion
1 9 24.3%
2 8 21.6%
3 or more 20 54.1%
Total 37 100%
24.30%
54.10%
21.60%
Figure 12: Duration of Hospitalisation
1 day
2 days
3 days or more
A majority (54.1%) spent 3 or more days in the hospital.
Patient Satisfaction with Intrapartum and Postpartum Nursing
Care: Buea Regional Hospital Annex.
4.1.6. Distribution according to
Parity Table 7: Distribution according to Parity.
PARITY Frequency Proportion
Primipares 17 45.9%
Multipares 20 54.1%
Total 37 100.0%
Figure 13: Parity Distribution
|
54.10%
|
|
45.90%
|
|
Primipars Multipares
|
54.1% of the participants were multipares.
4.1.7. Mode of Delivery Table 8:
Distribution according to Mode of Delivery.
MODE OF DELIVERY Frequency Proportion
Normal delivery 24 64.9%
Emergency C/S 13 35.1%
Total 37 100%
Figure 14: Mode of Delivery
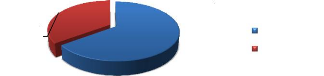
Normal delivery Emergency C/S
64.90%
35.10%
64.9% of the participants delivered per-vagina
4.2. Intrapartum Nursing Care Assessment 4.2.1.
Nurses' Attitude on Admission
Table 9: Distribution according to Nurses' Attitude on
Admission.
Attitude Frequency Percentage
Friendly and welcoming 31 83.8%
Not very welcoming 2 5.4%
Unwelcoming 4 10.8%
Total 37 100%
Majority (83.8%) said nurses were friendly and welcoming.
4.2.2. Nursing Comfort Measures
Table 10: Distribution according to Nursing Comfort Measures.
Comfort and Support? Frequency Proportion
YES 23 63.9%
NO 13 36.1%
Total 36 100%
Comfort Measure Frequency Proportion
Placing hand in anus 2 8.3%
Words of comfort 16 66.7%
Back rubs 1 4.2%
Medications 2 8.3%
Sensitisation 1 4.2%
Cautioning 1 4.2%
Prayer and counsel 1 4.2%
Total 24 100%
Most patients (63.9 %) benefited from comforting measures and
among them 66.7%
received words of comfort and encouragement.
4.2.3. Breathing Techniques Taught
Table 11: Distribution according to Breathing Techniques
Taught.
Received Teachings? Frequency Proportion
YES 20 60.6%
NO 13 39.4%
Total 33 100%
60.6 % received teachings on breathing techniques.
4.2.4. Environmental Hygiene
Table 12: Distribution according to Environmental Hygiene.
Environment Frequency Proportion
Clean 34 94.4%
Unclean 2 5.6%
Total 36 100%
Majority (94.4%) affirmed that the maternity was clean.
4.2.5. Time spent with patients
Table 13: Distribution according to Time spent with patients.
Time accorded? Frequency Proportion
YES 28 87.5%
NO 4 12.5%
Total 32 100%
How often if YES? Frequency Proportion
At regular intervals 11 39.3%
On emergency 4 14.3%
During examination and drug administration 13 46.4%
Total 28 100%
87.5% of the patients acknowledged that time was spent with
them during labour and
46.4% of this time was spent during examinations and
drug administration.
4.2.6. Interpretation of Patients'
feelings
Table 14: Distribution according to Interpretation of Patients'
feelings.
Interpretation? Frequency Proportion
YES 13 40.6%
NO 19 59.4%
Total 32 100%
A lesser proportion (40.6%) of the respondents had the
interpretations of their feelings
while 59.4% of them did not have.
4.3. Postpartum Nursing Care Assessment 4.3.1.
Monitoring Vital signs
Table 15: Distribution according to Monitoring Vital signs.
Vital signs checked? Frequency Proportion
YES 24 64.9%
NO 13 35.1%
Total 37 100%
How often if YES? Frequency Proportion
Regularly every 5 mins 2 9.1%
Every 30 mins 5 22.7%
Once a day 9 40.9%
Twice a day 5 22.7%
Immediately after delivery 1 4.5%
Total 22 100%
A majority (64.9%) had their vital signs checked and 40.9% of
such checks were done just
once daily.
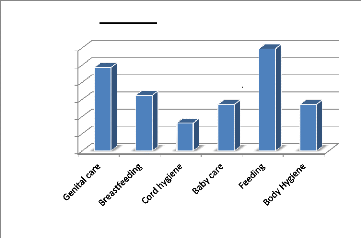
4.3.2. Patient Education
Table 16: Distribution according to Patient Education.
Topic Taught Frequency Proportion
Genital care 9 24.3%
How to breast feed 6 16.2%
How to care for baby's cord 3 8.1%
How to bathe/care for baby 5 13.5%
Feeding 11 29.7%
Hygiene 5 13.5%
Total 39 100%
Proportions
30.00%
25.00%
20.00%
15.00%
10.00%
0.00%
5.00%
24.30%
Figure 15: Patient Education
16.20%
8.10%
Topics Taught
13.50%
29.70%
13.50%
Education was mostly given on feeding (29.7%).
4.3.3. Examination of Baby
Table 17: Distribution according to Examination of Baby.
Baby examined? Frequency Proportion
YES 10 27.0%
NO 27 73.0%
Total 37 100%
How often if Yes? Frequency Proportion
At least once every shift 4 40%
Once a day 6 60%
Total 10 100%
Most babies (73.0%) were not examined postpartum. For the few
who were examined 60%
of such examinations was once daily.
4.3.4. Examination of Mother
Table 18: Distribution according to Examination of Mother
Mother examined? Frequency Proportion
YES 18 48.6.0%
NO 19 51.4%
Total 37 100%
Checks performed Frequency Proportion
Amount of bleeding 18 48.6%
Breast examination 11 29.7%
Genitals 5 13.5%
Conjunctiva 17 45.9%
Fundal height 11 29.7%
More than half of the population never had any checks at all,
and among such checks, 48.6%
was monitoring the amount of bleeding.
4.4. Assessment of Patient Satisfaction
4.4.1. Rating during Intrapartum (using the Likert's
Scale)
|
|
Table 19: Rating during Intrapartum
|
|
RATING
|
Mean Value
|
Frequency
|
Proportion
|
|
Very good
|
1
|
34
|
20.2%
|
|
Good
|
2
|
71
|
42.3%
|
|
Fair
|
3
|
42
|
25.0%
|
|
Poor
|
4
|
21
|
12.5%
|
|
Total responses
|
|
168
|
100%
|
|
RATING
|
Ability to give
Information
(%)
|
Care and
Concern
(%)
|
Skills and
Competence
(%)
|
Restful
Atmosphere
(%)
|
Coordination of
Care
(%)
|
|
Very good
|
14.7
|
18.9
|
24.2
|
18.8
|
25.0
|
|
Good
|
35.3
|
35.1
|
48.5
|
46.9
|
46.9
|
|
Fair
|
20.6
|
35.1
|
21.2
|
28.1
|
18.8
|
|
Poor
|
29.4
|
10.8
|
6.1
|
6.3
|
9.4
|
|
Total
|
100
|
100
|
100
|
100
|
100
|
Proportion
40.0%
60.0%
50.0%
30.0%
20.0%
10.0%
0.0%
14.7%
Ability to give
Information
35.3%
20.6%
29.4%
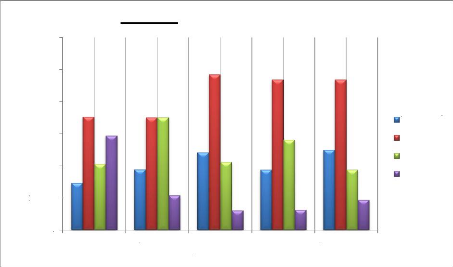
Figure 16: Rating during Intrapartum
18.9%
35.1%
Care and
Concern
35.1%
10.8%
24.2%
Skills and
Competence
48.5%
21.2%
6.1%
18.8%
Restful
Atmosphere
46.9%
28.1%
6.3%
25.0%
Coordination
of Care
46.9%
18.8%
9.4%
Very good Good
Fair
Poor
A greatest proportion of the respondents (42.3%) indicates that
the nursing care was good, that is; 35.3% for good nursing ability to pass on
information, 35.1% for good nursing care and concern, 48.5% for good nursing
skills and competence, 46.9% for a good restful atmosphere and coordination of
care. Thus giving a Mean value of 2.3 and a standard deviation of
(ä=0.9).
4.4.2. Rating during Postpartum(using the Likert's
Scale)
|
Table 20: Rating during Postpartum
|
|
RATING
|
Mean Value
|
Frequency
|
Proportion
|
|
Very good
|
1
|
10
|
7.1%
|
|
Good
|
2
|
48
|
34.0%
|
|
Fair
|
3
|
30
|
21.3%
|
|
Poor
|
4
|
53
|
37.6%
|
|
Total responses
|
|
141
|
100%
|
|
RATING
|
Information
given
(%)
|
Nursing
attention
(%)
|
Responsiveness
to calls
(%)
|
Reliable
services
(%)
|
Recognition of
opinions
(%)
|
|
Very good
|
0.0%
|
11.1%
|
9.9%
|
6.9%
|
3.9%
|
|
Good
|
20.0%
|
30.6%
|
46.7%
|
41.4%
|
26.9%
|
|
Fair
|
10.0%
|
25.0%
|
16.7%
|
17.2%
|
34.6%
|
|
Poor
|
70.0%
|
33.3%
|
26.7%
|
34.5%
|
34.6%
|
|
Total
|
100%
|
100%
|
100%
|
100
|
100%
|




46.7%
34.6%
34.6%
|
Proportion
|
70.0% 60.0% 50.0% 40.0% 30.0% 20.0% 10.0% 0.0%
|
80.0%
70.0%
20.0%
10.0%
0.0%
30.6% 33.3%
25.0%
11.1%
26.7%
16.7%
9.9%
41.4%
34.5%
17.2%
6.9%

26.9%
3.9%
Information given Nursing attention Responsiveness to
calls
Reliable services Recognition of
opinions






Very good Good Fair Poor


Figure 17: Rating during Postpartum
A majority of the respondents (37.6%) indicated that the
postpartum nursing care was poor, that is; 70% for poor nursing ability to
communicate, 33.3% lacked nurses' attention and 34.6% of patients' opinions
were not recognized. However, for the 34.0% who rated the care given as good,
46.7% had good response to calls and 41.4% for good reliability of nurses to
perform their services. Thus giving an overall Mean value of 2.9 and a standard
deviation of (ä=1.0).
4.5. Patients' Recommendation of the
Maternity
The respondents made recommendations solely based on the nursing
they received.
|
|
Table 21: Patients' Recommendation of the Maternity
|
|
Recommendations
|
|
Mean values Frequency
|
Proportion
|
|
Strongly agree
|
1
|
9
|
25.0%
|
|
Somewhat agree
|
2
|
19
|
52.8%
|
|
Somewhat disagree
|
3
|
4
|
11.1%
|
|
Strongly disagree
|
4
|
4
|
11.1%
|
|
Total
|
|
36
|
100%
|
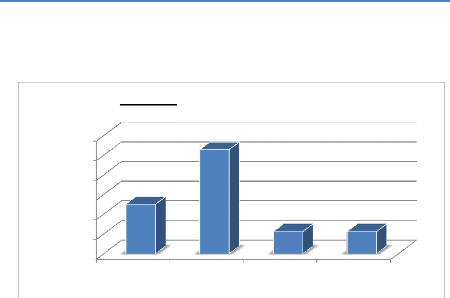
Strongly disagree
Strongly agree Somewhat agree Somewhat
disagree
Figure 18: Patients' Recommendations
52.8%
60.0%
50.0%
Proportions
40.0%
25.00%
30.0%
20.0%
10.0%
0.0%
11.10% 11.10%
A majority of the respondents (52.8%) somewhat agreed to
recommend the Maternity to their family members and friends. Hence giving an
overall Mean value of 2.1 and a standard deviation of (ä=0.9).
4.6. Patients' Opinion on how satisfaction can be
improved.
The chart below represents various ways on which patient
satisfaction can be improved based on the patients' perspective.
Table 22: Patients' Opinion on how satisfaction can be
improved.
|
PATIENT'S OPINION
|
Frequency
|
Proportion
per
Individual
|
Proportion
on total
answers
|
|
Authorities should sanction stubborn nurses
|
1
|
3.4%
|
1.7%
|
|
Bathe babies and improve on child care policy
|
10
|
34.5%
|
16.7%
|
|
Be more comforting and caring
|
7
|
24.1%
|
11.7%
|
|
Be more friendly, polite and truthful
|
11
|
37.9%
|
18.3%
|
|
Be understanding, respectful and collaborate with patients
|
7
|
24.1%
|
11.7%
|
|
Improve on mother care policy
|
15
|
51.7%
|
25.0%
|
|
Improve on hygiene and mend toilets
|
3
|
10.3%
|
5.0%
|
|
Improve on number of nurses for rapid intervention
|
3
|
10.3%
|
5.0%
|
|
Teach what patients don't know
|
3
|
10.3%
|
5.0%
|
|
TOTAL
|
60
|
|
100%
|
|
DISCUSSION, CONCLUSION AND
RECOMMENDATIONS
5.0. Introduction
From the preceding chapters, we have reviewed literature on
labour and delivery, postpartum, the nurses responsibilities during these
periods and measuring quality of care using patient satisfaction. From the data
collected and analysed, the results will be discussed in this chapter related
to the above sub topics. Discussion therefore is on demographic data, nursing
care offered during intrapartum and postpartum periods, and patients
satisfaction with the care given and ways in which patient satisfaction can be
improved.
5.1. Discussion of results
5.1.1. Choice of study area
Our study area was the Buea Regional hospital Annex, it was
chosen because it is acting as a teaching hospital and is expected that the
care given to the patients here should be standard. Also it acts as a referral
point for health centers patients coming from all over, it is relatively
cheaper thus receives more people than any other health service in the Buea
locality. Assessing patients' satisfaction will help to improve the nursing
care in this great unit of the hospital.
5.1.2. Socio-Demographic Findings
The mean age was 26 with the most represented age group being
20-25. This could possibly be justified by the fact that the most fertile
period in a woman's life is when she is between 22-30 years old. The mean age
for the study population falls between this age group.
Majority of the population (47.1%) had FSLC as their highest
level of education with most of them being low income earners. 34.3% of them
(housewives and applicants) had nothing doing. The study population was made up
of people with low level of education and low social class because the more
educated and better placed people prefer to go to other healthcare providers in
or out of town. Many participants (17.1%) were students.
A greater proportion of the study population constituted
married women while (32.4%) were single. The high rate of sexual activity
during the late teenage and early adolescent ages as well as increased sexual
promiscuity nowadays could possibly account for the high proportion of single
mothers in this study.
54.1% were multipars while 45.9% were primipars. Though most
of them 64.9% had their babies per vagina, a high percentage (35.1%) had their
babies through emergency caesarian section. The fact that the hospital is a
central referral unit could probably account for this.
Most of the patients (54.1%) had spent more than three days in
the hospital. This could be explained by the fact many patients so desired to
voluntarily prolong their stay.
5.1.3. Nursing Care Findings
A) During Intrapartum.
According to the data collected, it could be seen that most of
the women, 83.8% were welcomed in a friendly manner. This implies that the
nurses in this unit generally are soft and have a warm attitude towards their
clients. This addresses the psychological aspect of care since knowledge and
technical ability only are insufficient [33].
Concerning provision of comfort, a majority 63.9% said the
nurse provided them with comfort measures this shows that the nurses here have
some concern and empathy for their patients. With most of them giving words of
comfort, 8.3% were given analgesics and another 8.3% said they had anal touch
which made them feel more comfortable.
Most of the patients received teachings on how to breathe in
and push. Though this is mostly done in the antenatal clinics it is important
to do it in the labour ward as this is an important aspect in the management of
labour [31].
94.4% said the maternity was clean and once again highlights
the importance of environmental hygiene in nursing care.
As for the time spent with patients, 46.4% said nurses spent
time with them during emergencies or when called, 39.3% said nurses spent time
with them during drug administration while only 14.3% said nurses spent time
with them at regular intervals. This demonstrates that the nurses are hardly
always by their patients and so only see them when they have a procedure to
carry out. This is not a positive nursing attitude since constant presence is
very vital [35].
In this study, 59.4% of the respondents said the nurses did
not interpret the meaning of their feelings to them and this could possibly
explain the high levels of patient dissatisfaction. Conlusively, the nursing
care offered during intrapartum is average.
B.) During Postpartum.
In the study, it was discovered that only 64.9% of the women
had their vital signs checked after delivery. A great proportion of 45.1% never
had their vitals checked. Only 33.6% of the study population had their vital
signs checked regularly or 30 minutes after delivery. This is poor nursing
practice as the first four hours after delivery is a critical period and vital
signs are an important indicator of adverse changes [25].
From this survey it was observed that postpartum teachings
were very poor as more than half of the patients were not taught anything. Only
24.3% had teachings on how to care for their perineum, 16.2% were taught how to
breastfeed their babies, 8.1% were taught how to care for the umbilical cord,
13.5% of the population were taught how to bath their babies, 29.7% were taught
on good feeding habits and only 13.5% were taught on hygiene. All these show
the lack of zeal in postpartum follow-up and care.
After delivery, both the mother and the baby will have health
concerns that need to be addressed attentively [31] but from the analysis of
the data collected, 73% of the babies were not examined. Of the 27% who said
their babies were examined, 60% had their babies examined just once a day. Thus
the babies were not being given full attention.
Concerning postpartum checks done on the mothers, 48.6% were
checked for bleeding and this proportion is quite small considering the
complications of postpartum haemorrhage. A small proportion 29.7% had their
breasts examined. This proportion is too small as women who could have breast
engorgement or breast infections will not be easily identified and possibly
screened for breast cancer [31]. Only 13.5% had their genitals examined.
Genital examinations are very important in evaluating postpartal adaptation
[23]. Blood loss during the birth process is common and so checking the
conjunctivae will be indicative if the woman is anaemic. Paradoxically only
45.9% had their conjunctivae checked. 29.7% of the women were checked for
uterine involution which was not enough.
From the above analyses it can be concluded that the mothers and
their babies are not well followed up after delivery rendering postpartum
nursing care poor.
5.1.4. Patients' Satisfaction with Nursing
Care
A.) During Intrapartum.
Five indicators were used to determine patients satisfaction
with nursing care: Nurses' ability to inform patients, Nursing concern and
care, Nursing skill and competence, A restful atmosphere provided by the nurse
and the coordination of care.
In this study, the majority (35.3%) rated the nurses ability
to pass on information as good, 20.6% as fair ,24.9% as poor and 14.7 % as very
good. This implies that the majority were fairly satisfied with the information
they received. This is a true picture because if we relate it to the
information they were given during this period, most of them (60.6%) were
taught breathing techniques as seen on Table 11 and many of them
(40.6%) did not have explanations of what they were going through as shown on
Table 14. From the suggestions the patients gave, the attitude of the
nurse or mode of passing on the information too could be a factor which will
rate the information as being fairly satisfactory.
For Nursing care and concern, an equal majority 35.1% rated it
good and fair (fairly satisfied and fairly unsatisfied) while 10.8% were
unsatisfied. Summarily, more people (54%) were fairly satisfied .This could be
explained by the fact that many women (63.9%) were given comfort measures
during the pain and difficulty they went through. (See Table 10)
As concerns the skill and competence of the nurse, a majority
rated it good meaning that they were fairly satisfied. Also a large proportion
(24.2%) rated it very good implying that they were satisfied with the nurses'
skill. From the nursing care given, majority said the nurse was there to
administer their medications and respond to emergencies. This is in line with
most studies which indicate that the nurse focuses on tasks [33].
Most respondents rated nurses' ability to provide a restful
and quiet atmosphere as being good. This is justified by the 94.4% of the
patients who acknowledged that the labour ward was clean as shown on Table
12.
For coordination of care, most of the respondents (46.9%)
rated the teamwork spirit of the nurses as good, 25.0% as very good, 18.8% as
fair and 9.6% as poor. This brings us to the conclusion that the respondents
were fairly satisfied with the coordination of care.
A Likert's scale was drawn for the six points and the Mean
value gotten signified that the nursing care was good. This implies that the
participants were fairly satisfied with the care they received during the
intrapartum period. Hence more effort must be put in so as to fully satisfy the
patients.
B.) During Postpartum.
The indicators used were information given to the patients,
nurses' attention towards patients, nurses' responsiveness to calls, nurses'
reliability to perform services and recognition of the patients' opinion.
As concerns the information given to them, 70% of the
population rated it poor. This implies that they were unsatisfied with the
information which was given to them. 20% rated it good, 10% fair and no body
rated it very good. Their dissatisfaction was due to the fact that little or no
information was given to them at postpartum. From Table 16, 29.7% of
the population had a teaching on at least one subject among whom only 24.3%
were taught on genital care and only 16.2% on breastfeeding despite the fact
that 45.9% of the population were primipara with little or no experience on
this. A few were taught on how to care for the baby's umbilical cord. 13.5%
were taught on baby's care, 29.7% of them were taught on good feeding habits. A
majority of them were those who underwent caesarian sections and were
restricted from solid meals. This is in line with studies which prove that
patients value value postpartum information [7].
From the data collected, 46.7% of the respondents rated the
nurses' ability to respond to calls as good. This implies that a good number of
the nurses attended promptly to the calls of their patients. Though a good
proportion 26.5% said they were unsatisfied with the way the nurses responded
to their calls. This implies that most of the patients were fairly satisfied
with the nurses ability to respond to calls.
Majority of the patients were fairly satisfied with the nurses
reliability to perform services but a large proportion (34.5%) were
dissatisfied with the nurses' reliability. 17.2% were fairly unsatisfied with
the nurses reliability. A minority (9.9%) were satisfied with the reliability
(see Table 20). From this, we could conclude that the respondents were
fairly satisfied with the nurses' reliability.
For nurses involvement of the patients to the care, it was
generally unsatisfactory as 34.6% graded their involvement as poor and 34.6%
graded it as fair . Very few of the patients (26.9%) rated their involvement as
good and a small proportion (3.9%) were satisfied with their involvement. From
a recent undefended thesis , more patients want to participate though the
nurses do not encourage them [38]. This is could certainly account for their
unsatisfaction.
Patient Satisfaction with Intrapartum and Postpartum Nursing
Care: Buea Regional Hospital Annex.
From the data collected and analyzed , a Likert's scale was
developed and the mean value gotten which was approximately 3 and was
considered fair. This implies that most of the respondents were fairly
unsatisfied with the care offered at postpartum.
5.1.5. Patients' Recommendation of the Maternity
service
The patients were asked if they will recommend the maternity
based solely on the nursing care which they had received. The mean value gotten
corresponded to a majority who somewhat agree to recommend the maternity to
their family members and friends. This anchors the fact that the respondents
were generally fairly satisfied with the nursing care provided.
5.1.6. Ways to Improve Patient Satisfaction
In the opinion of the respondents, in order to increase
patient satisfaction with nursing care, nurses should improve on patient
education, mother and child care policy, comfort, care and understanding
measures. This is similar to a research done by Lomoro and collaborators in
2002 on improvement of quality of care where emphasis were laid on health
education on childcare.
5.1.7. Testing of Hypothesis
Testing of hypothesis depends on the data that was collected.
The hypothesis reads «Patients receiving intrapartum and postpartum care
in BRHA are not satisfied with the nursing care they receive.»
From the data collected, it is evident that the participants
were fairly satisfied with the intrapartum nursing care and unsatisfied with
postpartum nursing care. Overall, they were fairly satisfied with nursing care
and thus, the hypothesis is valid.
Patients will be more satisfied if nurses can employ measures to
reinforce postpartum care.
5.2. Conclusion
For most women, intrapartum is usually a time of excitement,
anticipation, anxiety fear and pain while postpartum is a time for
physiological and psychological adjustment for both the mother and her baby.
The nursing care offered to them should be one which is safe, positive and
satisfying to the mother.
From the research, participants were fairly satisfied with the
care offered to them during intrapartum. This is because the nurses were
generally friendly and welcoming, patients were taught breathing exercises,
were supported and provided with a clean environment. Contrarily, participants
received minimal care offered during postpartum and were therefore
dissatisfied. The overall patient perception with the nursing care offered by
this maternity service was fairly satisfactory.
The participants further suggested that in order for their
care to be more satisfactory, nurses should improve on the information they
give their patients, their attitude towards patients and the zeal for their
work.
Nursing care should thus be improved on in order to improve
patients satisfaction.
5.3. Recommendations
v' Nurses in this unit should have refresher courses for the
care of their intrapartum and postpartum patients so that they will be able to
increase their knowledge on proper care of these patients.
v' The hospital should implement regular checks on the nursing
care given to patients that the nurses will have a sense of duty
consciousness.
v' Studies on patient satisfaction should be done in the other
units of the hospital so that a global change is done to improve care in this
hospital.
v' Government should recruit qualified staff to ensure quality
care is given to patients.
For further research
1. Factors responsible for the low quality of nursing care
offered during postpartum.

1. W.H.O. Basic Document. 1992. 39th edition.
2. Mollas Donaldson. Measuring the Quality of
Healthcare. 1999. National Academy Press Washington D.C.
3. Page L.A. The new midwifery science and
sensitivity practice. 2000. Churchill Livingston Imprint of Elvier Ltd.
4. Shields Donna. Nursing Care in Labor and
Patient Satisfaction, a descriptive study. Journal of Advanced
Nursing, 1999. 3(6) 535-50.
5. Guzzetta Cathie E. Essential Readings in
Holistic Nursing. 1998. Aspen publishers.
6. Lisa P. Patient compliance and satisfaction
with nursing care during delivery and recovery. Journal of Advanced
Nursing, 2002. 16(2) 60-66.
7. Lin C. Patient satisfaction with nursing
care as an outcome variable dilemma for Nursing evaluation researchers.
Journal of Professional Nursing, 1996. 12(4) 207-216.
8. Newhouse R., Poe S. Measuring Patient
Safety. 2005. Jones & Barlette Publishers, London.
9. Janet C. Perception of childbirth experience
and its relationship to early postpartum parenting. Journal of Advanced
Nursing, 1999. 8 (10) 1257-1264.
10. Bryatin J. Women's perception of Nursing
support during labor. Journal of Obstetrics & Gynaecology and Neonatal
Nursing, 2006. 23(8) 638-44.
11. Peterson W.E., Sward W., Charles C.
Adolescents' perception of inpatient postpartum Nursing Care, a
qualitative health research. 2007.
12.
www.indexmude.com
13. W.H.O. Department of making pregnancy safe. 2004.
39th edition.
14. Woodward C.A. Strategies for Assisting
Health workers to modify and improve skills. 2000. Oxford university press, New
York USA.
15. W.H.O. Developing World has acute shortage of health
workers. 2007.
16. Perla T. Patient compliance and
satisfaction with care during delivery and recovery. Journal of Nursing
Care Quality, 2003. 10(8) 56-60.
17. Philips Celeste. Family centered Maternity
care. 2003. Jones & Barlette Publishers, London.
18. American Academy of Pediatrics and the American
College of Obstetricians and Gynecologists: Guidelines for Perinatal
Care, 5th ed. 2002. Washington, DC, AAP and ACOG.
19. American College of Obstetricians and Gynecologists
Committee Opinion No. 267: Exercise during pregnancy and the
postpartum period. 2002. 99:171. ACOG.
20. Bernal AL: Overview of current research in
parturition. 2000. 86:213.
21. Kilpatrick SJ, Laros RK. Characteristics of
normal labor. 1989. 74:85, [PMID: 2733947]
22. Cohen W, Friedman EA (eds). Management of
Labor. 1983. Baltimore, University Park Press.
23. Mayerhofer K, Bodner-Adler B, Bodner K, et al.
Traditional care of the perineum during birth: A prospective,
randomized, multicenter study of 1,076 women. Journal of Reproductive
Medicine, 2002. 47:477, [PMID: 12092017].
24. Berman Mimi Cohen C. Obstetrics and
Gynaecology, 2nd ed. 1997. Lippincot Williams & Wilkins Company
Ltd. publishers U.S.A.
25. Simpson K.R., Creehan P.A. Perinatal
Nursing, 3rd ed. 2008. Lippincot Williams & Wilkins Company Ltd.
publishers U.S.A.
26. Delaune, Suc C., Lander P.K. Fundamentals
of Nursing Standards and Practice. 1998. Delmar publishers, U.S.A.
27. Hobfol S. E. Stress, Social support and
Woman. 1986. Hemisphere publishing corporation.
28. UNICEF/OMS/FNUAP. Guidelines for Monitoring
the Availability and Use of Obstetric Services. 1997. UNICEF: New York.
29. FNUAP et AMDD. Reducing Maternal Deaths:
Selecting Priorities, Tracking Progress, Distance Learning Courses on
Population Issues. 2002. Turin: UN System Staff College.
30. W.H.O. Standard classification of hypertensive disorders in
Pregnancy. 2003.
31. Littleson V. Lynna, Engebretson Joan C.
Maternity Nursing Care. 2009. Plengane Learning Publishing
Corporation, Canada.
32. Rosdah C. B. , Kowalsi M. Textbook of basic
Nursing, 9th ed. 2008. Lippincot Williams & Wilkins Company Ltd.
publishers U.S.A.
33. Dujardin B, De Schampheleire I, Sene H, et al:
Value of the alert and action lines on the partogram. 1992. Lancet
339:1336, [PMID: 1350000]
34. Williams A.M. Quality measurement.
Journal of Advanced Nursing, 1998. 27(4) 808-816.
35. Corbett C.A., Callister. Nursing support
during labor. Clinical Nursing research. 2000. 9(1) 70-83.
36. Bryatin J. Womens' perception of Nursing
support during labor. Journal of Obstetrics & Gynaecology and Neonatal
Nursing, 2006. 23(8) 638-44.
37. Merlyn D. Harris. Handbook of Home Health
care administration. 2005. 4th ed. Jones & Barlette Publishers
International Barbhouse, London.

I am Chwinui Mbeinkong, a final year nursing student of
the department of nursing in the University of Buea. I am carrying out a
research on patient satisfaction with nursing care offered during and after
labour and delivery. The information required from you is strictly for academic
purposes. I will be very grateful if you make an effort to answer each question
honestly. All information will be treated with confidentiality. Thanks for your
cooperation
Please put a tick ( ? ) where necessary or fill the
blanks where appropriate.
Section A. Socio-demographic Data
1) Age:
2) Educational level: FSLC O/L A/L Degree
others
3) Marital status:
4) Profession:
6) How many days have you been in the hospital? 1 2
3 or more
8) How many times have you been pregnant?
....................................
9) Mode of delivery: Normal vaginal Caesarean
section
Section B. Nursing care
? During Labour and Delivery
1) How did the nurse treat you on admission?
A) Friendly and welcoming B)not very welcoming C)
unwelcoming
2) Nurse provides comfort and support during pain and
discomfort? YES NO
If yes what did she do?
4) Were you taught how to breathe and how to push? YES
NO
6) Were you provided a clean environment? Yes NO
8) Did the nurse spend time with you in the labour
ward? YES NO
If yes, how often?
At regular intervals On emergency During examination
10) Did the nurse help you to interpret the meaning of your
feeling and showed concern?
YES NO
Dear Respondent,
7) Were your vital signs checked immediately after
delivery? YES NO
If yes, how often?
Regularly, every 5mins. Every 30mins. Once daily twice
daily.
? After Labour and Delivery
APPENDIX 1: DATA ENTRY FORM
1) Information: how clear and complete
were the nurse's information about what you were going through?
2) Concern and caring by the nurses:
Courtesy and respect, friendliness and kindness?
3) Skills and competence of the nurse: How
well were things were done?
4) Restful atmosphere provided by the nurses:
Amount of peace and quietness?
5) Coordination of care: team work between
the nurses and other staff?
II. After Delivery
6) Information given: Concerning breast
care, perineal care, breast feeding?
7) Attention of nurses to your condition:
how often did the nurses checked on you?
8) Nurse's responsiveness to calls: How
quick were they to respond to your calls?
9) Reliability to perform promised services
10) Recognition of your opinion: how much
you were involved (participated) in decision making?
Section C. Patient Satisfaction
Please rate some things about the nursing care offered
during your hospital stay in terms of whether they were very good ,good, fair
or poor.
I. During labour and delivery Very
Good Good Fair Poor
8) Which of the following topics did the nurse teach you
on?
Genital care
How to breast feed
How to care for baby's cord How to bathe/care for baby
Feeding Hygiene Others
10) Did the nurse come around to examine (physical assess)
the baby? YES NO
If yes, how often?
At least once every shift once a day more than twice a day
12) Which of the following checks did the nurse do?
Amount of bleeding Breast examination Genitals
Conjunctiva
Height of uterus Others
Based on the nursing care I Strongly Some what Some what
Strongly
Will recommend this maternity agree agree disagree
disagree
To my family and friends
Section D. Possible ways of improving patient
satisfaction patients
In your opinion, perspective what should the nurses do in order
to improve the quality of care and make you more satisfied.
THANK YOU!!!
APPENDIX 2: CONSENT FORM
| 

