B.3.1. First Stage of Labour:
The duration of the first stage of labour in primiparous
patients is noted to range from 6-18 hours, while in multiparous patients the
range is reported to be 2-10 hours. The lower limit of the normal for the rate
of cervical dilatation during the active phase is 1.2 cm per hour in first
pregnancies and 1.5 cm per hour in subsequent pregnancies.
The latent phase is prior to the active phase and last 6-8
hours. The cervix dilates from 0 to 3-4cm. The length of the cervix shortens
from 3cm to less than 0.5cm long.
The active phase begins when the cervix is about 4cm dilated and
ends at full dilatation (10cm).
The Transitional phase is from 8cm dilation until expulsive
contractions are felt by the woman.
B.3.2. Second Stage of Labour:
The second stage generally takes from 30 minutes to 3 hours
in primigravid women and from 5-30 minutes in multigravid women. The median
duration is 50 minutes in primipara and 20 minutes in multipara.
The transition period between the first and second stage is
marked by more frequent contractions and often server pain. Symptoms are
increased in bloody show and a feeling of pressure on the rectum accompanied by
a desire to bear down with each contraction. The descent of the fetus also
called the station, is evaluated to assess the progress of labour. It is done
by measuring the relationship of the bony portion of the foetal head with
respect to the maternal ischial spines. According to ACOG, when the bony
portion of the foetal head is at the level of the ischial spines, the station
is 11011.
The mechanism of labour in the vertex position consists of
engagement of the presenting part, flexion, descent, internal rotation,
extension, external rotation, and expulsion of the baby in this chronological
order.
B.3.3. Third Stage of Labour:
This is the stage of separation and expulsion of the placenta
and its membranes. It usually last for 2 hours in primigravids and 1 hour for
multigravids. Separation of the placenta generally occurs within 2-10 minutes
by the end of the second stage, but it may take 30 minutes or more to
spontaneously separate.
Signs of placental separation are:
v' A fresh gush of blood from the vagina.
v' The umbilical cord lengthens outside the vagina.
v' The fundus of the uterus rises up.
v' The uterus becomes firm and globular.
When these signs appear, it is safe to place traction on the
cord. The gentle traction, with or without counter-pressure between the
symphysis and fundus to prevent descent of the uterus, allows delivery of the
placenta.
C. The Postpartum Period (Puerperium)[23]
The puerperium consists of the period following the delivery of
the baby and placenta to approximately 6 weeks postpartum and further
classified as:
- Immediate Postpartum 4 Birth to 24 hours
- Early Postpartum 4 24 hours to 1 week
- Late Postpartum 4 1 week to weeks
The immediate postpartum period is a critical time for both
maternal and neonatal physiologic and emotional adjustment. It is during this
time that most postpartum complications occur.
C.1. Different phases of postpartum [17]
The postpartum period has three phases:
· «Taking in» phase:
During the taking in phase, which is within the first 24 hours after delivery,
physical recovery occurs. The mother is passive and dependent needing to be
mothered herself. She is fatigued after the hard work of labour and needs
nourishment, rest and sleep. However, she also needs her baby so that the
attachment phase can continue.
· Following the taking in phase, the woman goes through
the «taking hold» and «letting go»
phases. It has generally been accepted that these phases last 3 to 14
days each. In the «taking hold» phase, the woman gains control over
her body and assume her independence and autonomy. In the letting go phase, the
woman establishes new maternal role patterns.
C.2. Postpartal Systemmic Adaptations
A comprehensive nursing assessment is based on a sound
understanding of the normal physiologic process of puerperium:
C.2.1. Uterine Changes
1. Uterine Involution.
The uterus increases markedly in size and weight during
pregnancy (about 10 times the non-pregnant weight, reaching a crude weight of
about 1000 g) but involutes rapidly after delivery to the non-pregnant weight
of about 50 to 100 g at an average rate of 1cm/day.
Patient Satisfaction with Intrapartum and Postpartum Nursing
Care: Buea Regional Hospital Annex.
Immediately following delivery, the uterus weighs about 1 kg,
and its size approximates that of a 20-week pregnancy (at the level of the
umbilicus). At the end of the first postpartum week, it normally will have
decreased to the size of a 12-week gestation and is just palpable at the pubic
symphysis. During involution, the size of the cells decrease markedly but there
is no decrease in number. The outermost layer becomes necrotizing and is
sloughed off in lochia. Proteolytic enzymes promote autolysis except at the
placenta site [24]. Involution usually causes myometrial contractions or after
pains and last three weeks. Breastfeeding increases such contractions due to
further release of oxytocin. Mothers might need a first class analgesic.
2. Changes in fundal position.
Following expulsion of the placenta, the uterus contracts
firmly to the size of a large grape fruit. Walls of the uterus are about 4 to 5
cm in diameter. After birth, the top of the fundus remains at the umbilicus for
about half a day. On the first day following birth, the fundus is 1cm below the
umbilicus. The top of the fundus descends 1cm or a finger breath per day until
it descends into the pelvis about the tenth day [17].
3. Lochia .
One of the unique capabilities of the uterus is its ability to
rid itself of the debris and remains after delivery. This discharge, termed
lochia is classified according to its appearance and content:
v' Lochia rubra is dark red in color persisting for
2-3 days and contains erythrocytes,
epithelia cells, leukocytes, bacteria,
lanugo and occasionally fetal meconium [10].
v' Lochia serosa is pinkish to brownish. It flows
from about the 3rd day to 10th day composed of serous
exudates shreds of decidual erythrocytes, leukocytes, cervical mucus and
numerous micro-organisms.
v' Lochia Alba is composed of primary leukocytes,
decidual cells, epithelia cells, fat cervical mucus, cholesterol crystals and
bacteria [10].
Lochia has a stale musty odour which is not offensive.
4. Cervical changes.
Following birth, the cervix is spongy, flabby and formless.
It appears bruised but the original form of the cervix is regained within a few
hours. The cervical os admits two fingers for a few days following birth but
only one finger by the end of the first week. Change of shape of the os is
permanently changed by child bearing [24].
5. Uterine Vessels
Successful pregnancy requires a massive increase in uterine
blood flow. To provide for this, arteries and veins within the uterus, and
especially those of the placental site, enlarge remarkably, as they transport
blood to and from the uterus. Within the uterus, growth of new vessels also
provides for the marked increase in blood flow. After delivery, the caliber of
extra uterine vessels decreases to equal, or at least closely approximates that
of the pre pregnant state. Within the puerperal uterus, larger blood vessels
are obliterated by hyaline changes which are gradually resorbed, and replaced
by smaller ones.
C.2.2. Vaginal and Perineal Changes
Following birth, the vagina appears oedematous and may be
bruised. Lacerations may be present and rugae obliterated. The site of vagina
decreases and rugae returns to normal within 3 weeks. Soft tissue in and around
the perineum may appear oedematous with some bruising.
C.2.3. Mammary glands
After birth, the inter play of maternal hormones leads to the
establishment of milk production at the level of the mammary glands of the
breasts. This occurs through a series of mammogenesis (cellular multiplication
at the start of pregnancy) and lactogenesis (cellular differentiation by the
end of pregnancy).
Rapidly increasing Progesterone levels causes secretion of
prolactin, which in turn causes milk letdown to be effective within the first
(24-48) hours after delivery. Such breasts are usually swollen, tender and
febrile on touch.
Colostrum flows for about 5 days, which gradually becomes
converted to full milk by the 4th week.
C.2.4. Weight Loss
In addition to the loss of about 5 to 6 kg due to uterine
evacuation and normal blood loss, there is usually a further decrease of 2 to 3
kg through diuresis. Most women approach
their self-reported pre-pregnancy weight 6 months after delivery
but retain an average surplus of 1.4 kg
C.2.5. Urinary System
The postpartal woman has an increased bladder capacity,
swelling and bruising of the tissue around the urethra, decreased sensitivity
to fluid pressure hence at risk of over distention and incomplete emptying.
Urinary output increases during early postpartum due to puerperal diuresis
[25].
C.2.6. Gastro-Intestinal System
Hunger following birth is common and the mother may enjoy a
light meal. Frequently, she is thirsty and will drink large amounts of fluid.
Bowels tend to be sluggish after birth because of the lingering effects of
progesterone and decrease abdominal muscle tone [17].
C.2.7. Changes in Vital signs
During the postpartum period, with the exception of the first
24 hours, the woman should be afebrile. Blood pressure should remain stable and
within normal range following birth. Puerperal bradycardia with rates of 50 to
70 beats per minute commonly occurs during the first 6 to 10 days [26].
C.2.8. Others
Temporal amenorrhoea within 6-12 weeks in 100% of
non-breastfeeding mothers, and about 36 weeks in 70% of mothers carrying out
effective breastfeeding.
Ovulation occurs only after 40 days for non-breastfeeding
mothers and may extend right up to 6 months for breastfeeding mothers due to
the inhibitory effect of prolactin on FSH through a negative feedback
mechanism.
Hypercoagulability due to triggering of the intrinsic pathway
by thromboplastin, massively released in the course of placental detachment.
This poses a high risk of thromboembolic complications within the first 3 weeks
following delivery.
C.3. Postpartal Psychological Adaptations
C.3.1. Depression
It is common for a mother to exhibit some degree of depressed
mood a few days after delivery. This situation, termed postpartum blues,
describes a transient period of
depression that occurs in most women during the first week or
two after birth. It is manifested by mood swing, anger, weepiness, anorexia,
difficulty sleeping and a feeling of letting down. It is likely the consequence
of a number of factors:
v' The emotional letdown that follows the excitement and fears
that most women experience during pregnancy and delivery.
v' The discomforts of the early puerperium.
v' Fatigue from loss of sleep during labour and postpartum.
v' Anxiety over her capabilities for caring for her infant after
leaving the hospital. v' Fears that she has become less
attractive.
In the great majority of cases, effective treatment need be
nothing more than anticipation, recognition, and reassurance. This mild
disorder is self-limited and usually remits after 2 to 3 days, although it
sometimes persists for up to 10 days. Should postpartum blues persist or
worsen, a careful search should begin for symptoms of major depression, which
can occur in almost 20 percent of puerperal women [24].
C.3.2. Maternal Role
During the first two days, the woman turns to be positive and
somewhat dependent. Maternal role attainment therefore is a state whereby the
woman learns about her behavior and becomes comfortable with her identity as a
mother [17].
Although post partum period is a time of many physiological
and psychological changes, the stressors, they are usually considered good and
are not unhealthy [27].
C.3. Postpartum Complications
Several factors can hinder the normal physiological and
psychological puerperal evolution. Such complications greatly account for the
geometrically increasing maternal mortality in a developing country like
Cameroon from:
v' 430 deaths/100.000 in 1990
v' 669 deaths /100.000 in 2000
1' 1000 deaths/100.000 in 2010 [EDS 2010
(national statistics and demographic data)] Maternal
mortality according to WHO is the death of a woman when she is pregnant, in
labour or within the 42 days following termination of the pregnancy due to
obstetrical induced causes [28]. These values are relatively quite explosive,
with a woman dying each minute due to pregnancy complications [29].
These postpartum complications are:
1. Postpartum Haemorrhage: This is the leading
cause of maternal mortality (24.8%) and noticed in 5% of total pregnancies
worldwide [30]. It is defined as excessive bleeding greater or equal to 500ml
following a per vagina delivery. It is termed «severe» if values
exceed 1000ml. Possible aetiologies include:
v' Persisting uterine atony (70-90)%.
v' Obstetrical genital lacerations (cervical, vaginal and
perineal tears).
v' Retention of placental debris.
v' Others (retention of the entire placenta, haemorrhagic
endometritis, uterine inversion, uterine rupture, coagulopathies such as
DIVC).
2. Infection: Second leading cause of maternal
mortality after bleeding
(14.9%) [30]. The most common infectious causes of puerperal
fever include:
v' Endometritis usually due to premature rupture of
membranes.
v' Urinary infections (pyelonephritis).
v' Breast pathologies (lymphangitis, galactophoritis).
3. Pre-eclampsia / Eclampsia: Third major cause
of maternal mortality
worldwide (12.9)% and 25% of all eclampsia occurs during
postpartum[30]. Pre-eclampsia is a diastolic blood pressure greater or equal to
90mmHg measured 4hours apart (or 110mmHg in a unique measurement) associated
with a proteinuria of (0.3-5) g/l within 24 hours and occurring at a
gestational age at 20 weeks and above. Eclampsia is simply pre-eclampsia
associated with tonico-clonic convulsions [31].
4. Thrombo-embolic diseases: Usually are caused
by hypercoagulability.
Favourable factors include age (above 40 years), multiparty,
obesity,
dystocia or difficult labour, underlying cardiac pathologies
and past history of thromboembolic diseases. The most common manifestations are
pelvic phlebitis, superficial and deep venous thrombosis.
5. Anemia: Usually occurs following hemorrhage.
However, could also be Pre-existent. Characterized clinically by
cutaneous-mucosal pallor of the conjunctivae, gums, tongue, palates, palms of
the hands and soles of the feet. Biologically, it is a hemoglobin level less
than or equal to 10 g/dL in pregnancy.
Patient Satisfaction with Intrapartum and Postpartum Nursing
Care: Buea Regional Hospital Annex.
6. Puerperal Psychosis: Psychic disorders
usually during the late postpartum. About (1- 2)/1000 women who deliver suffer
from postpartum blues which when severe can lead to delirium, mania, depression
and other schizophrenic states [10]. Suicidal thoughts are not uncommon.
7. Puerperal Neuropathiess Characterised by
nervralgia, cramps and
Sometimes paralysis of the femoral and obturator nerves.
8. Spontaneous Symphysiotmy: This refers to
a disjunction of the pelvic bones at the pubic symphysis following delivery.
Clinically it is painful and normal function is impaired. On an x-ray, there is
a lateral luxation of the pubic symphysis as shown below.
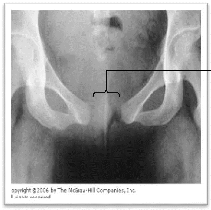
Figure 1:
An abdomino-pelvic x-ray (front view), showing a disjunction of
the pelvic bones following a
Lateral luxation
| 

