|

MADISON UNIVERSITY
BACHELOR FINAL PAPER
Model of organisation and functioning
of the socio educative district service for
the prevention and reduction of youth risk
and vulnerability to STI/HIV/AIDS in
Central African Republic
IN COLLABORATION WITH THE MINISTRY OF YOUTH, SPORTS,
ARTS AND
CULTURE AND NGO «AMBASSADE CHRETIENNE»
By : Supervisor :
Jeanne d'Arc KENGNE Dr. Badibanga N'Sambuka
Student N°: 21 90 38 HIV/AIDS Programme
Administrator
UNICEF
CONTENTS
|
No
|
TITLE
|
PAGES
|
|
PREFACE
|
3
|
|
ACKNOWLEDGMENT
|
7
|
|
LIST OF ABBREVIATIONS
|
8
|
|
LIST OF FIGURES
|
9
|
|
I
|
INTRODUCTION
|
10
|
I.1.
|
PROBLEMS
|
10
|
I.2.
|
FRAMEWORK OF THE CONCEPT
|
10
|
I.3.
|
|
DESCRIPTION OF THE CONTEXT
|
12
|
|
|
II.
|
GLOBAL APPROACH OF RISK PREVENTION PROBLEMS AND VULNERABILITY
OF THE YOUTH TO STI / HIV-AIDS IN THE THIRD SUBDIVISION OF BANGUI : OBJECTIVES
AND PROCESS
|
14
|
II.1.
|
OBJECTIVES
|
14
|
II.2.
|
|
PROCESS
|
14
|
|
|
III.
|
LIMITS OF THE PILOT EXPERIENCE
|
25
|
|
I.V.
|
RESULTS
|
26
|
|
V.
|
OPPORTUNITIES OF REPLICATION
|
41
|
|
V.I
|
CONCLUSIONS AND GENERAL COMMENTS
|
44
|
|
V.II
|
BIBLIOGRAPHY
|
48
|
Preface
It is with deep gratitude and total admiration of all people
who gave a contribution to the realization of this completely new pilot
experience under the technical guidance of the consultant Jeanne d'Arc Kengne,
namely the members of the Executive Educative Team, the young Supervising Peer
Educators of the pilot site and the Pastor Ambassador of the NGO
«Ambassade Chrétienne» that I write the preface of this book.
Since I took office at the Bangui Unicef Bureau in the Central African
Republic, in the month of March 2005, I have been dreaming of this most
creative application of my professional life and my knowledge of the
organization of district socio-sanitary services based on the system of primary
health care, then reproducing and adapting this model in a sector other than
health notably the socioeducative sector.
I was given an opportunity when it was assigned to me as one
of the major tasks to develop in the third district of Bangui a pilot
experience for prevention and reduction of risk and vulnerability of the youth
to STI / HIV/AIDS with their participation, to provide documentary resources
for this experience in view of making recommendations for the
generalization of the model to the whole country.
It was a mission to be entrusted to a research and training
institution in public health that would put at the disposal of the project a
team of experts for the development of such a pilot experience. However, this
was not the case. I thought it was judicious to fetch for services of an
individual, a person having experienced the idea being studied, able to assure
such a technical assistance while being member and supervisor of the team
responsible for the project at the same time, and moreover, to get the target
populations benefiting from the project involved as an indispensable resource
for its realization.
Right from the beginning, the problems of this pilot
experience have been focussed on the framework of the agreement to bear medical
costs of the populations in a participative approach having reached a level
where health structures are facing the fact that people's preoccupations for
their health are expressed in relation to their other preoccupations for a
certain well-being.
The approach implemented in the development, organization,
management and follow up of the project was based on a simple assertion:
«beginning from problems met at the level of health services / youth
population interface - discussing these problems with the youth - and, from
these problems thus mentioned (common place problems, local and / or isolated
ones, but truly felt) entering into bargain with existing structures in order
to «coordinate» the intersectorial action.»
The receptiveness and enthusiasm that the approaches developed
in this experience have given rise to are quite above our expectations and can
be considered with good reason as the true success of the model. After eighteen
months, the highest authorities of the country (The Presidency of the Republic
and the government) have adopted the model and have decided of its
generalization to the whole country.
Approaches developed in the course of this pilot experience
have confirmed, to us, two fundamental hypotheses of work in relation to the
participation of the population in the framework of integrating health system
as socio-economic sub-system in the political and administrative jurisdiction
(district, subdivision, council ...):
+ the integration of health preoccupations of the population
in a complete package representing its global preoccupations is accepted as
basic element on which the concept of participation rests
+ whatever the structures taking in charge the other
preoccupations of the populations, whatever their concepts, their objectives or
their methods, the type of interface they create at the level of the
populations, they influence these populations in one way or the other and then,
directly or indirectly, interact with the sanitary action.
The pilot experience in the third district of Bangui went
beyond our expectations; not only the work and contribution of the consultant
enabled to show that it was possible to repeat and adapt the sanitary district
model based on the primary health care system in the socioeducative sector, but
in addition, it gave another base of the approach in the development and
organization, management and animation of major strategic axes of a programme
for fighting against HIV/AIDS in accordance to the vision of the Medium Term
Strategic Plan (MTSP) 2006-2009 of Unicef.
Indeed the 4 Ps « la prise en charge pédiatrique
» (the agreement to bear medical costs in paediatrics), « la
prevention de la transmission mère-enfant du VIH » (the prevention
of mother -child transmission of HIV), « la prévention primaire
chez les adolescents / jeunes » (the primary prevention with adolescents
/the youth) and « la prise en charge des orphelins et autres enfants
rendus vulnérables par le fait du SIDA » (the agreement to bear
medical costs of orphans and other children made vulnerable due to AIDS) have
started to be discussed in an integrated way rather than vertical. The model of
the communication strategy for HIV/AIDS interventions based on the three
pillars (risk mapping, behavioural analysis and communication integrated plan)
combined to life skills being the federal element of the organization of the
agreement to bear medical costs of the 4 Ps.
The primary prevention with adolescents / the youth is stressed
in this model as the pivotal
and corner stone for the aspects of prevention
in the matter of fight against HIV/AIDS by the
fact that it opens a gateway towards the parent/mother - child
transmission prevention and its corollary the paediatric AIDS, for the youth
themselves are future parents or they become parents too early (mother
daughters / unmarried young mothers), towards the agreement to bear medical
costs of «OEV: Orphelins et Enfants Vulnérables» (orphans and
vulnerable children, children: in the street, children soldiers ...) for they
have a good knowledge of families having lost one or two parents and are often
the more concerned. The youth aged 10 to 24 make more than 40 % of the
population in the Central African Republic. Among pregnant women, those aged 15
to 24 have the highest rate of infection to HIV/AIDS.
I dare hope that the youth and their educators first, members
of the executive staff of ministries in charge of the youth and other
ministerial departments, leaders of national and international NGOs /
Associations, agencies of bilateral and multilateral cooperation as well as
those of the united nations system will find in this handbook a guide for an
integrated and participative approach of the prevention and reduction of risk
and vulnerability of the populations to HIV/AIDS in general and the youth in
particular.
Already, the youths of the pilot site are taking part to
international meetings and conferences to disseminate their experience and are
receiving other youths from other sites and countries (Burkina Faso) for
training and experience sharing visits.
Dr Badibanga N'Sambuka
MD, MPH
Acknowledgment
We couldn't have reached this stage of the work if UNICEF
Bangui hadn't accepted to entirely sponsor my consultation to carry out this
pilot experience. In this light we give special thanks to Dr FOUMBI Joseph the
former Resident Representative of UNICEF Bangui who without backsliding gave us
the technical support needed.
We expressed our sincere gratitude to Dr N'SAMBUKA BADIBANGA
of the UNICEF HIV/AIDS programme for his technical, scientific guidance and
coaching during all the steps of my course, to Dr Jean MACQ of the Public
Health School at the free University of Brussels (Ecole de Santé
Publique de l'Université Libre de Bruxelles) for cordial collaboration,
availability and advice despite his multiple occupations.
We are equally very indebted towards the representatives of
the ministries in charge of the youth and public health in the CAR, the NGO
«Ambassade Chrétienne» and in particular the supervising peer
educators, not forgetting the members of the Executive Educative Team for their
cordial cooperation that has led to the success of this experience.
We also express our gratitude and acknowledgement to the
members of «Association Culturelle Mission de la Re-Création»
(ACMR), in particular Jules Aigard NANFANG and Glory MOUKIA for their
suggestions, dialogue, translation and review of this handbook.
Our special thanks also go to our family members especially my
parents Mr and Mrs TAKAM Jean Marie in Yaoundé, and to my junior sisters
Noëlle Makouo and Josiane Koutsing for their moral support during hard
times.
We finally thank all the young peer educators of C.A.R who
have voluntarily and spontaneously accepted to sacrifice a little bit of their
time in order to contribute to the development of this pilot experience.
Special thanks to all the executive board of the Madison
University for the patience, devotion and particular attention that they have
shown through out the learning process.
Jeanne d'Arc Kengne
LIST OF ABBREVIATIONS
AIDS ASS CA CAR CBC CIEC EET
: Acquired Immune Deficiency Syndrome
: Associations
: Communication Area
: Central African Republic
: Communication for Behavioural Change
: Centre for Information, Education and Counselling
: Executive Educative Team
HC : Health Club
HIV LIP NGO NPSD PE
SPE STI
: Human Immune deficiency Virus
: Local Information Pool
: Non Gouvernemental Organisation
: National Plan for Sanitary Development
: Peer Educator
: Supervising Peer Educator
: Sexual Transmitted Infections
UNAIDS : United Nations Organisation for fight against AIDS
VG : Vulnerable Group
LIST OF FIGURES
|
Figure 1
|
:
|
Management diagram: global approach of health problems in the
development framework
|
|
Figure 2
|
:
|
Administrative map of the city of Bangui
|
|
Figure 3
|
:
|
Administrative map of the third subdivision of Bangui
|
|
Figure 4
|
:
|
Illustration of the organisation and functioning of socio-
educative services offered to the youth in the third district of Bangui
|
|
Figure 5
|
:
|
System working as an integrated complete package with possibility
of a dynamic interface with the youths population
|
|
Figure 6
|
:
|
Scheme of the Development activities
|
|
Figure 7
|
:
|
3 pillars of the strategy of communication
|
|
Figure 8
|
:
|
The spatial and demographic dimension
|
|
Figure 9
|
:
|
Needs, demand and supply
|
|
Figure 10
|
:
|
The Managerial dimension
|
|
Figure 11
|
:
|
The technical dimension
|
|
Figure 12
|
:
|
Model of organisation, management and animation of an integrated
district socio-educative service
|
|
Figure 13
|
:
|
PERT of the structural and functional organisation of the socio
educative district service
|
I - INTRODUCTION
I.1. PROBLEMS
In the plan of action for the 2005 - 2007 cooperation
programme between the Central African Republic and UNICEF, it was proposed to
develop in the third local council of Bangui a pilot experience for prevention
and reduction of the youth vulnerability to HIV-AIDS with their participation,
to document the experience in view of formulating recommendations for
the generalisation of the pattern in the whole country. The project was
intended to be a pilot site, and that implied a dual purpose:
1. to provide to the youth of the third local council the
ever best service in the limit of resources available («service»
purpose); not above the level of resources available in any medium size local
council of the CAR. It was a basic condition to prevent the pilot project from
degenerating into a masterpiece of academic bravery.
2. to turn the developed approaches into concepts («
research » purpose). To answer this purpose, the approaches developed in
the pilot site should be reproducible.
I.2. FRAMEWORK OF THE CONCEPT
The conceptual model below on the participation of the
population in the framework of health system integration as sub-system of the
local council socio - economic system has served as reference [1].
|
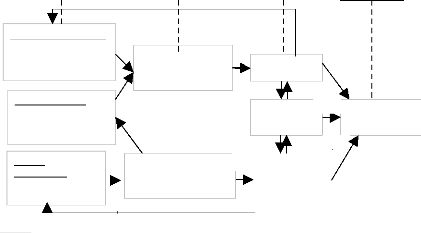
This diagram of management and animation shows that from
resources (relatively) limited and with considerable problems, a rational
management of health is a must. This means an efficient and effective
management.
Among available resources, there is the use of human
potential, which is indispensable in the increase of efficiency and
effectiveness of the treatment management. Health is not a general good in
itself; it only makes sens when seen as a contribution to human promotion. As
shown in the first diagram :
(a) Is the objective of health service and direct
contribution to development; (a) does not have any sense if:
(b) does not develop itself in parallel to it.
(c) Is the health service contribution by a non specific way
to development.
(d) Is the responsibility of a number of services among
which health service must be part.
However, for various reasons, the study of this interface did
not lay prior emphasis on research activities on health system.
|
Obstacles
Met
Methods to
use
Long term
objectives
Global aim
(d)
Figure 1: Management diagram:
global approach of health problems in the
Importance of problems HIV/AIDS -
M alnutrition - Transmissible diseases
Lack of opportunities
leading to a fatalistic attitude
Lack of resources Qualified personnel - finances-
furniture infrastructure - etc.
MEDICAL AND
HEALTH ANIMATION
M ANAGEM ENT Optimal use of resources
(Human resources)
(c)
GLOBAL SOCIAL A NIM ATION
&
SOCIO
ECONOM IC
DEVELOPMENT
Rise of the living standard
HEALTH
(b)
(b)
(a)
HUMAN
PROMOTION
Studies on the integration of population « health »
preoccupations in a huge complete package where other socio-economic structures
interact with the health action [1] have described how from problems met at the
level of the interface health service / population one can initialize a
dialogue with other existing socio-economic structures to
»coordinate» the inter sector action. The relation of the medical and
health animation with social animation (c) and socio-economic development (d)
can only express itself by «the integration» of the health system in
a whole complete package (figure 1) [1].
Other concepts range health and well -being in an ecologic
approach based on the principle that they are two intimately linked elements
and that they are determined by multiple conditions that interact on one
another (people's way of life, their social milieu the same as their
environment) [2].
In addition, studies on the analysis of various treatment systems
describe various models of integration system and how they can be coordinated
[3].
In reference to primary health care [4] and to health district
[5] [3] [6] as defined by the WHO, the participation of the populations is
erected as a pillar of health services delivery. The health centre is
considered as the element of the district health service whose specificity in
primary health care is to be the point of interaction between the service and a
defined community to which it delivers global health care, that is, complete,
continuous and integrated1 [5] [7].
Many studies also place the importance of participation in the
policy and practices for the promotion of health because it enables communities
to identify problems, propose solutions and favour change [8].
With the advent of AIDS pandemic, the youths are highly
exposed to the risk of contracting HIV. They are in the heart of this pandemic.
Their participation to HIV prevention programmes has been identified as being
an essential feature for the success of programmes that have recognized them
[9]. The participation of the youths to questions in which they are involved is
a right stipulated in the Convention of Rights of Children (CRC) [10].
I.3. DESCRIPTION OF THE CONTEXT
2
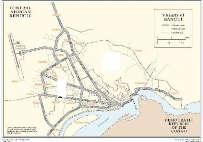
The pilot experience was developed in Bangui, the capital city
of the Central African Republic with an estimated population of 670,000
inhabitants divided up into eight districts. The third district covers an area
of 510 hectares with an estimated population of 134, 000 inhabitants among
which 53, 000 young people of 10 to 24 years old (40%). It is divided into two
groupings and twenty-nine quarters with eight main ethnic groups. The
socio-educative infrastructure comprises eight primary schools (among which
five are public), four Islamic
1 Comprehensive (whole) health care (globalité): illnesses
are considered in their total dimension (including social and economic
dimensions).
Continuity of health care: treatments are organized to follow
service users' right from the beginning to the end of their illness or their
risky episode as well as to follow the whole health needs of the community.
Integrated health care: promotion, prevention and education
activities are complementary to curative activities and they are integrated to
socio-economic development.
2 Data provided by the third district council of Bangui
schools for the study of the holy Quran, two secondary schools
(all of them public), two youth clubs, nine health centres (among which two are
public), an HIV voluntary testing centre, a sector for social action comprising
eight nursery schools (among which two are public), four catholic parishes,
twenty -two protestant parishes, six mosques, a police station, a gendarmerie
(French police station), a post and telecommunication service, a taxation
service, a « Crédit Mutuel de Centrafrique » desk, and two
playgrounds.
3
12
Figure 2 : The administrative map of
the city of
Bangui
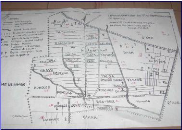
Figure 3 : The administrative map of
the third
district of Bangui
II. GLOBAL APPROACH OF PROBLEMS IN THE PREVENTION OF
RISK AND VULNERABILITY TO HIV/AIDS OF YOUTH IN THE THIRD DISTRICT OF BANGUI:
OBJECTIVES AND PROCESS
II.1.OBJECTIVES
Three main objectives have been defined in the framework of this
pilot experience:
1. to study the organisation-management conditions and
methods of the comprehensive responsibility (integrated, continuous and whole)
of youth risk and vulnerability related to STI/HIV/AIDS with their full and
active participation;
2. to exploit collected data for documentation ;
3. to provide to authorities in charge (of youth education)with
useful information for the generalisation of the model in the whole country.
II.2. PROCESS
In order to develop the pilot experience in the third district
of Bangui, activities undertaken or strategies used for information, education,
and counselling in matter of prevention and reduction of youth vulnerability to
STI/HIV/AIDS have been considered in certain cases as part of a more extended
district socio-educative system and in others as specific sub-systems.
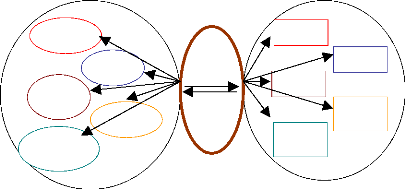
In this pilot experience, the analysis of basic
socio-educative structures and their constitutive
elements showed that socio-educative services were not structured in a system
but were made of a number of sub-systems not working as a complete package ;
there was no coordination among them and services offered to the youths were
scattered (Figure 4).
|
1. socio-educative services
|
|
2. target population
|
School youths
SCHOOL
SOCIAL SECTOR
Street children
YOUTH CLUBS
Youth out of school
HEALTH
CENTRE
Unhealthy youth or healthly
h
Youth
information centre
All the youths of the site
Figure 4 : Illustration of the
organisation and functioning of socio-educative services offered to the youths
in the third district of Bangui.
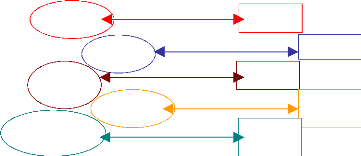
Consequently, a more efficient, effective and coordinated
structuration [11] was envisaged in basic socio-educative services - health
centre, youth club, social action sector, school, HIV voluntary testing centre,
youth friendly centre (CIEE in French) - organized in a system in such a way
that there are possibilities of creating a dynamic interface with the youths
(figure5).
|
1. socio-educative services
|
|
2. target population
|
Youth
information
centre
YOUTH CLUB
SOCIAL SECTOR
SCHOO
L
HEALTH
CENTRE
LIP
Youths out of school
All the youths of the site
Street children
School
youths
Unheathy youths or not
Figure 5 : System functioning as an
integrated comprehensive package with possibility of a dynamic interface with
youths population.
The LIP (Local Information Pool) would serve as element of
permanent interaction with the youths (figure 4) represented in different
structures of dialogue settled in the district which
are health clubs. This system will have to function as an
integrated comprehensive package3 offering information, education
and monitoring services (IEM or IEE in French) as a whole to the youths with
their full participation. It will be called « socio-educative district
system » made of basic socio-educative and referral services.
The approach followed relies on the replication of the model
of health district system based on primary health care. This model is indeed
the pertinent entity where various actors concerned by health domain can
envisage collaborating efficiently and acting to the adequate scale [12]. The
approach followed is systemic where the health district is conceived not as a
standard and catch-all modality of service organisation, but as a model to
adapt to circumstances, without forgetting the aim of a health service in the
urban context.
Thus, the model of health district has three essential
dimensions [12]. The first is spatial and demographic. It is
the definition of a precise population, living in a defined geographical zone,
corresponding or not to an administrative zone, on which the health authority
is responsible. This dimension of the model enables to introduce the notions of
zone of responsibility, health map, target population, and population
coverage.

The second dimension concerns the management and
authority functions. Exercised by the health authority, they range
from supervision activities and logistics to the financial management. This
managerial dimension4 of the model enables to re-examine the notions
of formal and functional authority, supervision and control, community
participation, and enabling of the inter sector action.
3 An integrated system of health is a system where elements
are organized, tidy and coordinated in view of common objectives: in our case,
it is the agreement to bear medical costs of problems related to prevention and
reduction of youth vulnerability to HIV/AIDS in the third district of Bangui
4 Management Functions, Chapter 1, page 11, Management
Fundamentals, Concepts-Applications-Skill Development. Robert N.Lussier, Ph.D.,
Springfield College, Springfield, Massachusetts, 2000 South -Western College
Publishing, a division of Thomson Learning.
The third dimension deals with organisation functions
concerning treatment, services and activities. This technical
dimension re-evaluates for the area the notions of users' circuit, services'
scales and relations among them, delegation or decentralisation of competences
and technology, or of reference system and counter reference system of patients
also.

The model of health district can be applied to the urban
context of the 3rd district without losing its coherence or abandoning its end:
the effective coverage of the population by Primary Health Care. [4]
The replication stages of the development and organisation of
such a system in a more extended socio-educative system are described in
documents of general policy, organisation, management, animation and training
designed during this pilot experience. Five strategic and operational axes have
been followed:

i. Development of an Executive Educative
Team.
To develop the various fields of activity of the pilot site,
an Executive Educative Team essentially made of volunteers identified and
chosen by the NGO «Ambassade Chrétienne» has been put in
place. Its members perform this social function without any remuneration other
than that of their habitual functions.
The Executive Educative Team exercising both technical and
administrative functions matching the profile of a social animator: teacher,
communicator, health professional, youth and animation councillor, and
management specialist.
|
The essential function of this team is the supervision of the
young supervising peer educators responsible of the organisation, management
and animation of the communication area (LIP, Health clubs). The structuration
in team and the work organisation have been a constant priority during the
whole process.
|
Health club in «castor» area of communication
Communication channels have been created to enable the
participation of everyone to the making of decisions
, tasks sharing, team spirit (responsibility in the group), and
the evaluation of activities through active research
from opinions of the others (meetings, folder for the circulation
of documents, calendar of activities, supervision notebook, etc).

Decisions were turned into « instructions »
preventing the member of the Executive Educative Team in charge of their
application of the pattern and the evaluation deadline. This has led to the
setting of a local information system containing management tools for the
organisation and functioning of the pilot site and a standard supervision
kit.
ii. Development of the coverage.
The global approach for the development of the coverage was
carried out at two levels: 1. Settlement of a basic socio-educative service
The council has been divided into 30 geographical units called
communication areas (CA), corresponding as much as possible to quarters
following the administrative structure (division). Each communication area is
under the responsibility of a young supervisor peer educator (SPE) and hosts a
local information pool (LIP), a potential space made up of 10 young peer
educators and a health club (HC) which pools representatives of youth
association (ASS) and vulnerable groups (VG) identified (street children, loose
girls, etc...).

In order to raise awareness for an individual search of
solutions to their problems, the social animation of youths is realised
throughout the health clubs considered as participation structures.

The local information pool has been organised structurally and
functionally to serve as interface between the participation and dialogue
structure of the youth (health club) and the basic socio-educative services.

The analysis/observation of the interaction between the local
information pool (LIP) and the health club on one hand, and the local
information pool (LIP) and the basic socio-educative structures on the other,
depending on the problem to solve, has permitted the understanding : + of
conditions to observe for the settlement of coordination and orientation
mechanisms of

the inter sector action ;
+ of each structure in terms of objectives to meet and minimum
package of activities to to

carry out;
+ of the technical, material and financial necessary support
related to the needs of youths.
Given the huge size of communication areas, alternative
approaches have not as yet been
developed to complement the coverage of the youth sub-urban
populations living at very
long distance from the local information pool (LIP): mobile
services of peer educators

for instance.

2. Establishment and rationalisation of the organisation
and functioning of a central structure as a Reference Information, Education
and Counselling Centre for basic socio-educative services. The Reference
Information, Education and Counselling Centre (Centre d' Information,
d'Education, et d'Ecoute des jeunes / CIEE in French) has been developed and
organised as a reference structure for the information, education and
counselling of youths in connection to the 30 local information pools. The
space organisation within the CIEE has been done taking into account the needs
in information and education (meeting room, library, video room), the needs in
management and follow -up of activities (office of the Executive Educative
Team),
|
1st stage
|
|
2nd stage
|
|
3rd stage
|
|
Transfer
|
|
Transfer
|
-Voluntary Testing -Behavioural analysis
-Risk
Mapping
- Census
Confidence
Quantita Rational
tive solutions
knowled to
ge of problems
problems studied
Continuous assessment and control system
Systematic study of priority problems

Identification and assessment of problems
IEC/CBC Treatment

the needs in management and follow-up of the equipment,
materials and furniture (store), the needs in the counselling of youths
(counselling room), the needs in management and follow up of activities in the
30 communication areas by the young supervisor peer educators (SPE room), and
the needs in training (conference room).


The functionality criteria, the composition, the localisation
and a standard kit of educative and didactic material for each socio-educative
structure («CIEE», LIP, and Health Club) have been defined.
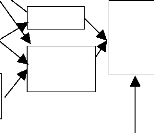
iii. Development of activities.
From the needs felt by youth population and with their full and
active participation, three complementary and simultaneous stages have been
followed in the development of activities:

|
Figure 6 : Scheme of the development of
activities
|
|
|
Transfer
|
First stage: choice of activities
Activities developed at the pilot site, which assures a well
defined geographical responsibility, were based on the three pillars of the
strategy of communication for behavioural change combined to life skills:
namely risk and vulnerability mapping, behavioural analysis, and integrated
communication plan, on one hand, and promotion of the use of condom,
orientation for
Risk and
vulnerability
mapping
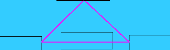
Life skills
Behavioural
analysis
Integrated
communication
plan
Figure 7 : 3 pillars of the strategy of
communication
counselling, HIV voluntary test, and, curative care and
professional insertion on the other
hand. These activities have been chosen depending on their
capacity to create
confidence in the youth population.
Second stage: study of identified problems
The quantitative knowledge of problems considered as priority
ones was acquired at three levels:
1. The identification and assessment of problems by youths
themselves ( meetings at the level of the LIP and the health club, risk and
vulnerability mapping, behavioural analysis , integrated micro communication
plan, social and health census).
2. The exchange between the youths and their supervisors on
the problems thus identified (Task Force meetings, restitution of vulnerability
and risk mapping, behavioural analysis, integrated micro communication plan,
health census).
3.


The members of the Executive Educative Team study at their
turn the problems rose by the youths or noticed by themselves during
supervisions and other visits on the field (Executive Educative Team
meetings).
·:. The management tools have been developed to allow
the collection, analysis, conservation and dissemination of data collected as
activities were implemented.
Third stage: research and application of solutions

The three levels instituted at the second stage, for a
systematic study of problems depending on priorities, have been used for the
research and application of rational solutions, specific to priority problems
identified and studied at the two previous stages. The information thus
collected have been used as they were made available, to progressively
rationalise the organisation of activities and to gradually developed basic
socio-educative services more specific to the pilot site ( meetings of the LIP
and health clubs, risk and vulnerability mapping restitution, behavioural
analysis, integrated micro communication plan, socio sanitary census).
iv. Progressive rationalisation of the internal
functioning of socio-educative structures of
the pilot site.
For practical and feasibility reasons, the application of new
approaches in the new structures has been given privilege over the internal
rationalisation of the functioning of previously existing structures. It did
not appear appropriate, at the risk of raising new needs for which the project
could not afford, to create new services, introduce new methods or techniques
without a previous study of their applicability, use and profitability in the
ongoing functioning of the previously existing socio-educative structures.


Methods and techniques that can enable the best coverage of
needs felt by the youths at the level of the pilot site have led the
organisation and functioning of the LIP and the «CIEE» + Implantation
and functionality criteria of the LIP and the «CIEE»
+ Choice of activities depending on problems considered as
priorities (Risk and
Vulnerability Mapping, Behavioural Analysis, Integrated
Communication Plan, Census,

Voluntary Screening Centre, distribution of condoms). + Meetings
of functional units
The « CIEE », the 30 LIP, and 30 health clubs have
been organised on the basis of promotional, preventive, curative or
socio-professional reinsertion functions to be fulfilled by the programme
around the following hypothesis of work:
·

:. The health club developed in the pilot experience is a
structure of participation. It is at this level that the integration of
«health» preoccupations of youth population in the comprehensive
package representing their global preoccupations is accepted as the basic
element on which the concept of participation is based.
· :. The interaction between the LIP and the health club
enables the coordination among different socio-educative structures in charge
of other preoccupations of youth populations and that interact with the health
action.
·


:. The LIP/ « CIEE » works as a global social
animation structure for the youths. The LIP, at the level of the communication
area, and the «CIEE» at the level of the whole council, are
structures of coordination and orientation of the inter sector action.

v. Promotion of the young peer educators as other human
resources of the population.
Given that human resources are limited, a policy of promoting
education by the peers has been conceived at the pilot site. This policy has
been based on a maximal delegation of tasks. Two convergent ways have been
used:
·


:. the standardisation of methods and techniques to make them
accessible to the young peer educators;
· :. the continuous training to upgrade their
competences.

The standardisation has been considered as part of the
rationalisation of activities while associating the peer educator in the
framework of their continuous training for the techniques that they have an
experience on.
The rise of the peer educators' competence was done in view of
a responsibility commitment based on an active training oriented towards
problems which they were facing. The 6 members of the Executive Educative Team
at the level of the « CIEE », the 30 SPE with 10 PE each at the level
of the LIP were pooled into teams corresponding to functional
service units sharing common objectives of work. 6 SPE represent
their peers in the Executive Educative Team. Each group meets regularly
following a well defined calendar. The aim of these meetings is to make
everyone become aware of the common objectives and individual responsibility in
their realisation, to define the assessment criteria and to evaluate the work
in a critical way in order to get to necessary improvements.
The situation study brought out the usefulness of reviewing
the knowledge necessary to understand certain problems and provided to each
team subjects to treat in a more systematic way. The holding of meetings
allowed informing peer educators bit by bit on general aspects of the project
to make them understand the framework in which they work so that they act as
intermediaries with youth population.

In this policy of promoting education by the peers, tasks were
delegated to the youths and their supervisors from the local population,
without a formal training, and ready to volunteer. Among the supervisors and
the youths trained through learning by doing, certain highly motivated and
skilled individuals emerged, being stimulated by the social function to
perform.
III. LIMITS OF THE PILOT EXPERIENCE
The notion of pilot site needs a double purpose, that of
providing services and that of research. Right from the beginning, a clear
definition of needs both of competent human and financial resources lacked. The
pilot experience has been conceived under the sole aspect of offering services
to the youth population using volunteers and not executive permanent paid
personnel for functions they exercise.
The NGO «Ambassade Chrétienne», partner in
charge of executing the pilot project, did not have own human and financial
resources. They depended entirely on the technical support and the financial
contribution of UNICEF to the extent that if these means could have not been
provided, they would have led to the collapse of the project.


The ministry of health which was in charge of the project at
the beginning was not in charge of the youth. It is in the course of the
execution of the project that the ministries in charge of the youth have been
implicated.
More over, the fact that at the UNICEF, there was no
substantial provision of means for the pilot experience delayed the development
process of different strategic and operational axes. The time allowed to
conduct such an experience ought not to have been restricted to the duration of
the annual cooperation action plan also.

The question of financing has not been taken into account as an
important development axis of the pilot experience of creating a district socio
educative service.
IV. RESULTS

The question we asked ourselves at the end of the 2007 annual
plan of action putting an end to the 2002 - 2007 programme cycle of cooperation
between the Central Africa Republic and UNICEF was to know whether the
replication of the health district model into a socio educative district and
its integration in a larger district socio economic system permitted to reach
the determined objectives.
(a).The study of conditions and organisation - management
methods of the integrated,
continuous and global responsibility to take in charge
risk and vulnerability of the
youths to STI/HIV/AIDS with their full and active
participation.
The same as for the health district, the notion of socio
educative district fulfilling the three essential dimensions. [13]
The spatial and demographic dimension

Notions of :
health map
target population
zone of geographic responsibility population coverage
Reference scale District health authority Health institution



Figure 8 : the spatial and demographic
dimension
The population has been well defined, living in a well limited
geographical area, the third district of Bangui, corresponding to an
administrative area. This dimension of the model has permitted to repeat at new
expenditures, the notions of area of responsibility, socio health map oriented
towards the risk mapping of the youth to HIV/AIDS, target population ( youths
of 10 - 24 years old) and of social, health and educative population coverage.
However, the major obstacle has consisted in having a unique social, health and
educative authority in
charge. The fact that the urban council district, considered
in the national health organisation as a health district, does not have a
health district head did not enable to put in place this control unit formally.
This notion of socio educative authority in charge of the structures of the non
formal educative system does not exist in the CAR, or if it does, is not
applied.

We did our utmost to make the third urban council of Bangui an
« area of responsibility » of a number of social, health and
educative institutions that accept to coordinate taking in charge health
problems of all youths aged 10 - 24 living there, whether they were already
using the services of those social, health and educative institutions or
not.


In fact, without an exact knowledge of youth population to
cover, of the area for which the local socio sanitary and educative system
accepts certain responsibilities, one did not know how: + to establish a full
social, health and educative coverage : how many youths of 10 - 24
years old one is in charge of ? What effort still to be made in
order to cover all youth
population through information, education and counselling,
treatment or activities of
diverse nature?
+ to conceive a realistic planning : how to evaluate needs,
which priorities, which volume of activities to foresee, which conditions of
implementation to envisage?
+ to undertake an evaluation of services : which common bases
(denominators) to take into account when one measures activities and results ?
What social, health and educative information system to put in place to collect
pertinent data and, in particular, succeed to get access to individuals
belonging to the target population?
+ to favour the community participation : with which authorities
one should dialogue, with which groups of the « civil society »,
which youths in which quarters, till which geographical limits?
+ to put in place the inter sector collaboration : with which
services ? Implicating which leaders? Mobilising which actors? Till which
physical limits?
The five elements above have been for us important arguments
used to make the district socio educative site match the youth population and a
given geographical area, that of the third urban council of Bangui. Throughout
the process the high importance of the social, health and educative coverage
should be noticed.
Demand
CBC
Real
Needs
In fact, the knowledge of the youth population by the district
socio educative system have enabled not to answer passively to the need
Offer of
Participation Rationalisation
Service
felt
Needs
of information, education and counselling, treatment and services
deriving from the youths. But it has enabled to be «pro-active»
and to look for means to make needs
demand and offer meet.
Figure 9 : Needs, demand and offer
AS
P
P
P
The management dimension
Notions of :
Formal and informal authority community participation
inter sector action
supervision and control
P = Population; AS = sectors other than health
Figure 10 : The management dimension
It is the management and authority functions. At the pilot
site, these functions have been exercised in an informal and functional way by
the Executive Educative Team without any socio educative and health authority.
The members of this team have achieved activities of supervision. The logistics
and the financial management being exercised by the supervising
NGO. This managerial dimension of the model has enabled to
re-examine the notions of formal and functional authority, supervision and
control, community participation and of dynamisation of the inter sector
action.
|
The technical dimension
|
Notions of :
+ users' circuit
+ delegation of tasks
+ scales of services
+ reference and counter reference
|
|
Figure 1 1 : The technical dimension
It deals with organisation functions regarding activities of
information, education and counselling the young people, treatment and
services. It has enabled to re-evaluate for the urban pilot site the notions of
circuit of the young people as users, scales of socio - educative and health
services, then the relation between them, delegation or decentralisation of
competences and technology, or of reference and counter reference system of the
youths asking for services (whether they are ill or not) also.
At the end of the year 2007, to scrutiny, the adequacy much
sought after becomes evident between this model and the functions assigned to
the mastery of a coherent and performing health district and socio educative
space. Conceived this way, we wanted the socio-educative district as well as
the health district to be more than a tool for Information, Education and
Counselling (IEC) organisation, treatment or socio-educative and health
services. It has become a pertinent entity where diverse actors concerned by
the field of the youth health can envisage to collaborate efficiently and act
at the adequate level.
|
Différent
actors
|
Différent relations et Différent
interactions Functions
|
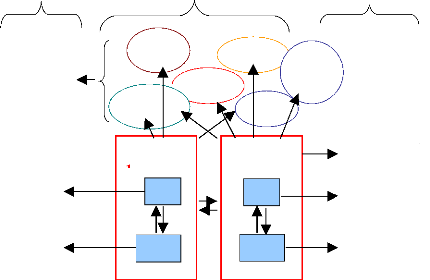
Youth association and vulnerabe groups
Pool of the
young peer
educators
Inter sector
Team
CA
Youth
information
center
HC
Youth Healh
club Center
LIP
Social
sector
HC
LIP
School
CA2
HIV voluntar y testing centre
Communication area (peripheral planning unit)
Coordination and orientation structure of the young peer
educators
Youth dialogue and
participation structure
Figure 12: model of organisation, management and animation an
integrated district socioeducative service
(b) The second objective dealt with the exploitation of
information collected in view of
the documentation of the pilot experience.
Right from the beginning of the pilot site development
different activities have been shared into « projects ». This
repartition was done essentially in accordance with the two fundamental
approaches of public health: the vertical approach (strategies of action
answering a problem - diverse methodologies)5 and horizontal
approach (organisation and rationalisation of services)6.
So, reproducing and adapting the organisation of the local
health information system, given
the vocation of the pilot site that is to
say with a dual aim namely « service delivery to
youths » and
« research », it has been put in place methods and techniques of
collection,
5 Projets symboliséd by figures
6 Projets symbolised by a set of three letters
analysis and conservation of information. These different
«projects» have been shared among different members of the Executive
Educative Team at the level of the pilot site.
A system of classified sheets in a folder of each project
enables to follow its evolution and make a report about its progress. Each
project is followed and documented in terms of: (see picture below).
> General principle (GP)
> Empirical decision (ED)
> Administrative instruction (AI) > Operational Instruction
(OI)
> Evaluation analysis (EA) > Evaluation instruction (EI)
> Evaluation monitoring(EM) > Basic data (BD)
> System (SYS)
> Progress report (PR)
This type of organisation has been conceived much more for the
management and follow up of the pilot experience and less for the organisation
of everyday routine of the members of the Executive Educative Team. This
responsibility was devoted much to the technical assistance assured by UNICEF.
This has enabled to conceive and elaborate tools for the management and follow
up of the development of the organisation and functioning of a normal site
offering socio educative and health services to a given population (see pilot
site documents
entitled «système d'information local -
SIL»).
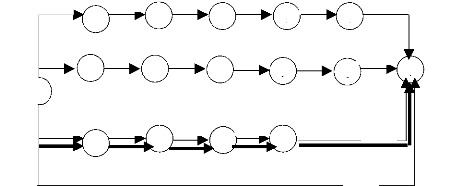
The application of the planning method based on Performance
Evaluation and Review (PERT) has enabled to piece together activities and
events that has contributed to the realisation of the specific objectives of
the pilot experience as shown in the figure 13 below.
B-1 F-3 E-3 J-3
A-1
K-1
5 8 1 1
2
C-1
D-1 H-2 L-1 N-3
R-1
3
6 9 1 1 1
End
Start
1
I-3 G-3 M-3 O-1
7 1 1
4 3
P-12
Q-12
Figure 13 : PERT of the structural and
functional organisation of the socio-educative district service
Path


1 2 5 8 11 14 16

A-B-F-E-K-J: 1M + 1M + 3M + 3M + 3M + 1M = 12 months
Path
1 3 6 9 12 15 16
B-D-H-L-N-R: 1M + 1M + 2M + 1M + 3M + 1M = 9 months
Path
1 4 7 10 13 16
I-G-M-0-P: 3M + 3M + 3M + 1M + 12M = 22
months
1 16
Q 12 M = 12 months
Path
Notes: Circles = Events; Arrows and letters = Activities;
Numbers = Time in month, Double arrows = the critical path, or how long it
should take to complete the project.
Following the PERT, multiple activities developed at the pilot
site are for some independent because they can be performed simultaneously;
others are dependent because one activity might be completed before the next
activity can begin. PERT is more appropriate the activities follow both
dependent and independent series of each other. Key PERT components are
activities, events, periods/time, the critical path and if possible the cost
[13].
The critical path determines the length of time take to
complete a project by determining how long each activity will take. In our
case, it is shown by the double line in Figure 13. 18 activities /events have
been followed for the realisation of the specific objectives of the project for
the structural and functional organisation socio-educative district service:
The Youths Centre for Information, Education and Counselling (YCIEC), the
Executive Educative Team (EET), the Supervisor Peer Educators (SPE), the Peer
Educators (PE), the Local Information Pool (LIP) and Health Clubs (HC):
A. Discussion with partners implicated (1 month)
B. Choice of the place of location of the CIEC (1 month)
C. Identification and training of the EET (1 month)
D. Identification and training of the 30 SPE (1 month)
E. Division of the site into communication areas and their
development (3 months)
F. Settlement and equipment of the CIEC (3 months)
G. Risk and vulnerability mapping (3 months)
H. Identification and training of 10 PE by each SPE (2
months)
I. Organisation and structuring of the EET team work (3
months)
J. Structural and functional organisation of the CIEC (3
months)
K. Preparation and Official opening of CIEC (1 months)
L. Implementation and organisation of the LIP (1 month)
M. Carrying out of the behavioural analysis and acquisition of
life skills (3 months)
N. Organisation and structuring of health clubs (dialogue
structure) 1 by communication area (3 months)
O. Elaboration of integrated communication micro plans by
peer educators in each communication area and the integrated communication plan
of the whole pilot site by members of the EET (1 month)
P. Implementation of micro plans of action in each communication
area by peer educators and of the plan of action of the site by members of the
EET(12 months)
Q. Supervision of the implementation of micro plans of action in
communication areas by the EET and the SPE (12 months)
R. Evaluation of integrated communication micro plans and of the
integrated plan of the site (1 month)
The estimative duration for each activity /event has been
determined (A-1, B-1, F-3, E-3, J-3, K-1, C-1, D-1, H-2, L-1, N-3 R-1, I-3,
G-3, M-3, O-1, P-12 and Q-12 the same as the sequence of realisation of
different tasks: (A is completed before B can begin, E before H, H before J and
so on... Q is an independent activity).
Management tools have enabled to get both better organisation
and follow up of services offered (service aim) and better knowledge of
priority problems and their solutions (research aim). Three categories of tools
have been conceived:
+ At operational level
Management tools are connected to the established socio
educative system which comprises two essential elements:
The basic socio educative service represented by the
LIP in this case considered as the functional unit of the pilot site
of IEC delivery in a dynamic interaction with the youth population of the
communication area covered represented by the health club.
A that level, management tools conceived enable:
· manage the problems of any youth (individually);
· manage the LIP in terms of minimum package of activities
to carry out;
· manage relations between the LIP and the youth
/population
Central reference unit: the CIEC where management tools
are used to:
· manage the CIEC in terms of structural and functional
organisation of a service offering a minimum package of activities to the youth
population of the whole pilot site ;
· manage relations among elements of the urban council
socio educative system (LIP and CIEC)
+ At the research level
The elaborated management tools enable to undertake research,
follow up and evaluation that is to say, to improve the delivery of socio
educative services by bringing new knowledge.
+ At the strategic level
Management tools enable to pile useful information and
dispatch them to the institution concerned and to give an orientation to the
general policy of planning, norms and procedures connected to the IEC delivery
to the youth population of the urban council.
(c) Bringing useful information to the authorities
concerned for the generalisation of the
model to the whole country.
Through out the pilot site development process, ministries
implicated in the prevention and reduction of HIV/AIDS youth vulnerability to
have been engaged in the framework of the cooperation programme between the CAR
and UNICEF. Thus, the ministry of public health assured at the beginning the
supervision and coordination of the project through the National Committee of
AIDS Control (Direction Nationale de lutte contre le SIDA - DNLS);
the ministry of youth has replaced the ministry of public
health ; the ministry of national education has intervened for the educational
part and the ministry of social affairs for social matters.
In each ministry, excepted that of social affairs, a
management team composed of three executives chosen by the minister assure the
technical support and the administrative management of the project following
the plan of action of the cooperation between the CAR and UNICEF.
A supervising committee made of representatives of each
management team to which the NGO «Ambassade Chrétienne», main
partner and responsible of the execution of the project and other youth
associations have been associated, assuring the global coordination of the
project. Since the youths are the target population, the presidency of the
committee, initially assured by the «DNLS» has been transferred to
the general Directorate of the Youth of the ministry of youth.
The implication right from the beginning, of executives of the
ministries in charge of the youths and the ministry of health has been of great
importance in the endorsement of the joint responsibility by those ministries
and UNICEF for the development of the pilot project. Factors that have
conditioned the development, the structural and functional organisation of the
district socio educative site in the third urban council by replication of the
health district model based on primary health care can be divided into three
main categories:
· Conceptual factors
· Political factors
· Factors connected to resources
1. C onceptual factors
The concept of reproduction and the reproductively character
can be understood in the
philosophical and global sense as a number of
institutional conditions. We will use it in a
more specific sense that is the measure in which a project
provides a certain number of precise answers to some problems, depending on
approaches that can be repeated elsewhere. It is not so much the conditions in
which these answers have been supplied that are important but the approaches
followed.
In the framework of the pilot experience of the third district
of Bangui, it has been established, right from the beginning, the
reproductively of concepts and methods as one of the justifications of the
action and the research.
Although the initial aim of the project was to study the
organisation of specific interventions in matter of prevention and reduction of
youth vulnerability to HIV/AIDS, this has been oriented towards how to assure
to the youth population of the third district the best service possible in
relation to available resources.
The CAR should be able to gain from this intervention
information and necessary material to define at national level, a policy and a
plan for promoting the youth health in general and for preventing HIV/AIDS
among them in particular. The constant preoccupation during the whole process
in view of its generalisation has been to draw conclusions for approaches
adopted and disseminate them.
The project has remained above all a project of health
promotion, even if other fields have been revealed important too. The
enlargement of the field of action to other fields of development such as the
socio economic re-insertion has just been envisaged with the active
participation of youths only. By limiting itself to the field of health
considered in a more global socio educative framework, the project has been
able to provide a certain number of precise answers regarding the organisation
of socio educative services in an administrative district corresponding to an
urban health district.
The concept of health district based on primary health care
that used to serve then as reference model was well understood. It has been
applied and extended to the district socio educative site where health has been
a sector with a very high technical component7.
From a conceptual point of view thus, to analyse the results
of the pilot experience, we have got to make use of the
«modelisation» of a district socio educative system, by conceiving it
in its merest form adapted to the health district system. It is a question of a
district socio educative system with two levels - a socio educative central
unit of reference (the CIEC) and socio educative peripheral units called Local
Information Pools (LIP). The model comprises three replicable dimensions: the
spatial and demographic dimension, the managerial dimension and the technical
dimension.
The conformity of the project to the national Policy of HIV/AIDS
control has been an important factor of success. The reference to the national
policy, legal arrangements, and other institutions that make its environment
has enabled the endorsement by the national authorities as well as actors on
the field of the project. There has been a very high mobilisation both at the
local and national level. The ministries of public health, youth, social
affairs and national education have accompanied the whole pilot site process of
development. The President of the Republic
Mr BOZIZE (see picture) and all the members of
government have visited the Youth Centre for
Information, Education and Councelling (YCIEC)
or «CIEE» in French).

2. Political factors
7 The health district versus the district socio educative site
roughly speaking can be defined as the functional unit of decentralisation of
the socio educative organisation for a well defined population. Its optimal
height and complexity in a given situation are the result of two opposed
requirements: it should be large enough to enable a certain concentration of
human and technical resources. But it should equally be small enough so as to
establish a communication with the population and a participation of
communities. In other words, the scale economy and the search of a bottom -up
planning must be reconciled to make treatment more pertinent in order to match
priorities. (ibidem, pp.7-8).
The position of leadership obtained by the HIV/AIDS programme
in the preparation of the (5th African Development Forum (ADF V) held in
November 2006 in Ethiopia, and in the organisation of the Youth National Forum
in December of the same year has led to the official adoption of the model and
the recommendation (by the authorities) of its generalisation to the whole
country.
3. Economic factors
To make the project less vulnerable, the following elements have
been taken into account: + the project has been based on principles of
simplicity and complexity,
+ realistic rather than global and integrated,
+ successive stages of realisation have been well defined and
are connected rather than being bound to be realised simultaneously,
+ by taking available resources as limit, the project has
prevented itself from the danger of realising a piece of academic bravery,
+ to concretise this will, several decisions have been taken:
the intervention unit of the project is the national planning unit of health
services that is the district, here the administrative district. The
development of the infrastructure is done with the volunteer personnel
available and by calling to the community participation for possible
improvements. The LIPs are managed by the youths themselves trained through
learning by doing.
4. The financing of the project.
In the present socio economic conditions of the CAR, featured
by the stagnation of the socio educative budget, that of health in particular
and the degradation of the purchasing power of the population, it was difficult
to make all the services of the pilot site finance by the state. It was also
unrealistic to expect the populations to finance the project by themselves. The
idea
right from the beginning has been to show that it was possible
to reproduce at low cost a taking in charge system of the prevention and
reduction of HIV/AIDS youth vulnerability by a socio educative service
following the organisation model of the health district.
Therefore, international aid has been considered as a
necessary solidarity to assure minimum services to the youth population so that
this aid should not create new needs. No new technique has been introduced
without its use being proved through a discussion within the team.
However, the question of financing should be discussed in a
further study in order to get the estimate of the investment cost and
functioning of district socio educative site offring services of information,
education and counselling to the youths in matter of prevention and reduction
of their vulnerability to HIV/AIDS.
V. OPPORTUNITIES OF REPLICATION
As mentioned above, we understand by replication the ability
for a project to provide answers to a problem following approaches that can be
repeated elsewhere and not the reproduction of all elements of the project.
Certain actions are dictated and highly influenced by the local context and
should not certainly be reproduced exactly as those undertaken somewhere else.
This is why, for example, standard instructions of risk and vulnerability
mapping and behavioural analysis are made to answer problems of the youth
population of the third urban council with means available locally. Repeating
them as such somewhere else would lead to inconsistencies and inefficiency.
What is replicable in this case is not the final product, but rather the
methodology of its elaboration and standard instructions for the young peer
educators.
However, and whatever the value of approaches, channels of
communication that enable to assure the dissemination of the experience must be
used.
a) The teaching of HIV/AIDS in schools
Teaching is an important mean for disseminating ideas.
Unfortunately, during the experimental stage of the model, it was not envisaged
to introduce the teaching of HIV/AIDS in school milieu of the fundamental level
2 following new approaches of life skills combined to the communication for
behavioural change as it was the case for fundamental level 1. However, the
consideration of the CIEC («CIEE» in French) in the national policy
of the youth, could bring to the teaching of youth animation in the framework
of the future National Center of Youth and Sports (NCYS, in French CNJS)
concrete field elements, by reinforcing the credibility of the education by
showing that ideas defended are achievable.
However, activities of prevention and reduction of youth
vulnerability to HIV/AIDS have
been introduced as extracurricular
activities. We have tried to complement and compensate
this lack of education by publications notably the description
of methods followed (example: the promotion of the young peer educator) or the
dissemination of key ideas such as the district socio educative service.
The presentation of the CIEC model («CIEE» in
French) at the «Ecole de Santé Publique de l'Université
Libre de Bruxelles» (School of Public Health of the Free University of
Brussels) in June - August 2006 has been an important stage as channel of
replication that should be maintained under a given form. The pilot site being
in itself a replication of the experience lived in Cameroon, it is as such a
good opportunity to test, improve and disseminate the methodologies
developed.
b) The training of national executives
At the end of the experimental period in 2007, although short
(24 months), the pilot site of the third urban council of Bangui has been
oriented as demonstration and reference site for the whole country. Therefore,
it has been planned to make it a training centre for national executives of the
ministries of youth and of national education. The contribution of national
executives of the CAR to the implementation of the project has been and will
continue to be an opportunity of training on the field and acquisition of an
important expertise.
c) To test approaches and methods
Very quickly, testing methods developed in the third urban
council of Bangui in-of- school and in the divisions (rural areas and emergency
in 2007) have got the double advantage of studying not only the replication,
but the acceptability of the methods in- school also and equally in the rural
milieu. Moreover, the approaches and methods applied at the pilot site are
themselves a replication of what has been developed in Douala in Cameroon.
d) Necessary conditions for replication
Definitely, the pilot experience of Bangui has enabled to define
three necessary conditions to the replication of these approaches:
The first observation that has been made is that it is
very difficult to seize the essence of an approach when one has not witnessed
all its beginning.
The replication in the school milieu of Bangui and division
(rural areas in 2007) has been indispensable to the understanding of the origin
of an instruction and its evolution in order to be able to remove anything
particular in it, but to understand its «raison d'être» also
before adapting it correctly to a different environment.
The second observation is connected to the difficulty
to interpret an approach and to the difficulty to discriminate the importance
of the detail. We have seen both at the pilot site of the third district and in
the school milieu that these difficulties have led to blocks and deviations.
The third observation made indicates that the methods
that have been the most easily adopted are those that corresponded to the
expressed needs both in the third urban council of Bangui and in the school
milieu. It has been generally a matter of fields in which there were questions
on how to operate. For example, the nationalisation of the organisation and
functioning of the Youths Centre for Information, Education and Counselling
YCIEC (»CIEE» in French), the risk and vulnerability mapping, the
behavioural analysis and the integrated communication plan. This observation
underlines the necessity of introducing as priority the methods that answer the
demand of people interested. In fact, the comprehension is easy if we answer a
problem rather than if we want to test a theoretical hypothesis.
VI. CONCLUSIONS AND GENERAL COMMENTS
The main weakness of the national socio educative and health
system in general, and in particular of the non formal education in the CAR as
in many developing countries lays in the absence of an adequate model of the
organisation of non formal education, out of the school system. The word model
is understood here in the sense of the reference organisational structure in
relation to which diverse variations are defined.
The structures of the ministry of youth in the CAR are
distinguished nowadays by the existence of official youth services badly
equipped without maintenance and very often not functioning on one hand, and by
the desperate efforts deployed to create, despite everything, new structures
that do not answer national realities on the other. The model of organisation
of youth socio educative and health services, as a mirage, continues to raise
hope and important expenditures with in most of the cases disappointing
results. We are totally in front of a poverty of the non formal education. This
poverty is not only linked to the present economic climate that is to say
linked to the lack of personnel and adequate infrastructure, poor supply,
equipment and management conditions of youth socio educative and health
services, but to the failure of the adaptation of the model inherited from the
colonial period also. There is a deeper vacuum, a conceptual vacuum.
In this documentation, we have described an organisation model
of information, education and counselling of the youths in the framework of
HIV/AIDS control but from a sector other than health while borrowing from the
latter the simple organisation model of two complementary scales in which all
curative and preventive activities are integrated, which is adapted to socio
economic conditions of the third urban council of Bangui. This model could then
fill an important conceptual vacuum.
In the poor functioning conditions of youth services, many
supervisors of the youths and policy makers think that, the improvement of
services should pass through the progressive rehabilitation of existing
structures as resources are made available. Such an approach although a bit
easy, still has many inconveniencies, the most important of them being the
difficulty to make the youth population and the personnel of youth animation
perceive that socio educative services for the promotion of the youths do not
mean « earning a bit more» but changing the nature of services.
It is preferable to define the model of basic socio educative
services that we want to settle in the area. The interest is that we start from
a clear reference obliging each time to justify possible variants.
The analysis of the use of this simple system shows that it is
satisfactory and enables to take efficiently in charge the problems of
prevention and reduction of youth vulnerability to HIV/AIDS both in and out of
the reference service, the CIEC (»CIEE» in French). However, the main
constraints must be taken into account and two of them influence the
application of the model in the CAR:
> the important degradation of the country economic
possibilities that make it more and more dependent on foreign aid for the
financing of its socio educative and health services.
> the lack of competent human resources to assure the
spreading and implementation of the model.
The simple model described offers to the CAR one conceptual
framework of planning, organisation and implantation of non formal socio
educative structures playing a role in the care of youth problems notably the
prevention and reduction of their vulnerability to HIV/AIDS.
The existence of the model presents many advantages:
a) A framework for international assistance
By making this model adopted in the whole CAR, a framework
has been created in which actions and resources can be driven giving them a
great coherence to the planning of the non formal socio educative action.
b) A framework for national coordination
The existence of the functional model in town as well as in
the rural milieu will create coherence not only for foreign donors but for
various actors in the country also. The model, by highlighting the functions of
each scale, will enable to reach a better coordination among actors. They feel
more concerned by the youth population health which they are responsible of in
the framework of a policy (for the promotion of the youth, of health).
c) Moderator effect on certain constraints.
A weakness of the realisation of care in CAR is the lack,
after having divided the country into health districts, of a coherent national
plan that defines stages of realisation of this model, one health district
after another, in some words a national «pre-plan». For the youth non
formal socio educative sector, there is no «pre-plan» too. The latter
could offer a flexible reference framework that could enable to decide
depending on pre-established criteria rather than on diverse pressures.
It should be unrealistic to think that the existence of a
conceptual model lifts the constraints to the realisation of the National
Health Development Plan based on the policy of primary health care for the
health sector. However a conceptual model gives a better base to get to more
relational solutions in a given political context. As the experience of the
pilot site of the third urban council of Bangui shows it, this model, by
filling a conceptual vacuum creates a framework in which political options of
the country are concretised and enables to avoid that the organisation of non
formal socio educative services are turned into a Babel tower.
Moreover, there is good reason to underline here that the
participation of the population that of the young people in particular, is
raised as the corner stone of the successful completion of the project. The
socio educative and health structures animated by the young people (CIEC, LIP,
Health club) have enabled to undertake activities at the community level, to
give an orientation and to coordinate the inter sector action at basic level.
However, even if it has been demonstrated that it was possible to develop
activities of prevention and reduction of youth, vulnerability to HIV/AIDS with
their full and active participation, it is also true that if the other socio
educative sectors that should provide answers to problems which the youths are
facing are not organised in the same perspective, an important link in the
chain could lack and then the objectives targeted will be far from being
reached.
VII. BIBLIOGRAPHIE
1. P.Mercenier, Equipe du Projet Kasongo : « document
de travail : participation de la population dans le cadre de
l'intégration du système de santé comme
sous-système socio- économique zonal à Kasongo »,
1987.
2. Lise Renaud, Mauricio Gomez Zamudio, préface de D.
Green, Planifier pour mieux agir, Extraits choisis, Montréal, REFIPS,
1998, pp. 1-58
3. Rifkin, A.B, Muller, F. and Bickhman, W. (1988) Primary
health care: «on measuring participation» Social Science and
Medecine, 9, pp931-940.
4. OMS-FISE (1978). Les Soins de Santé Primaires.
OMS, Genève
5. OMS (1987). La Déclaration de Harare, le District
de Santé. OMS, Genève.
6. Deborah Ritchie, Odette Parry, Wendy Gnich, Steve
Platt:» Issues of participation,
ownership and empowerment in a community development
programme : tackling
smoking in a low - income area in Scotland, Health Promotion
International,
Vol.19.No.1, Oxford University Press 2004.
7. P. Mercenier, le rôle du centre de santé
dans le contexte d'un système de santé de district basé
sur les soins de santé primaires. Institut de Médecine Tropicale,
Anvers, 1988.
8. Blackburn, J. (2000), Understanding Paulo Freire :
reflections on the origins, concepts and possible pitfalls of his educational
approach. Community development Journal, 35, pp 3-15.
9. Programmes Nationaux de Lutte contre le Sida : «
Guide des indicateurs de suivi et d'évaluation des programmes nationaux
de prévention du VIH/SIDA pour les jeunes ». Organisation Mondiale
pour la Santé, 2004, pp35.
10. Unicef, programme Division, : «The Participation
Rights of Adolescents: A strategic
11. Ronald M.Andersen, Thomas H.Rice, Gerald F.Kominski:
Changing the US Health Care System, Key Issues in Health Services, Policy and
Management, 1996, pp 13-56
12. Daniel, Grodos, page vi, dans district sanitaire urbain
en Afrique subsaharienne.
13. Robert N. Lussier, Management Fundamentals : Concepts -
Applications Skill Development, 1999, page 163-164.
| 

