II.5) DIAGNOSIS OF MENINGITIS IN CHILDREN
II.5.1) CLINICAL DIAGNOSIS OF MENINGITIS IN
CHILDREN
The clinical symptoms and signs of bacterial meningitis in
children vary depending on the age of the child and duration of disease. The
classic symptoms of meningitis are fever, headache, photophobia and neck
stiffness. However, in the early stages of meningitis, and particularly in
young children, the symptoms of meningitis can be variable or nonspecific and
the classic symptoms may be absent, making meningitis difficult to diagnose.
Nonspecific signs include abnormal vital signs such as tachycardia and fever,
poor feeding, irritability, lethargy, and vomiting [23][
39].
Children may have fever and vomiting associated with
irritability, drowsiness and confusion. They may become suddenly ill with fever
and rigors, which can be mistaken for seizures. Also muscle and joint aches can
occur which can be responsible for children being restless and miserable.
Vomiting, nausea and poor appetite are common while abdominal pain and diarrhea
are less common. Meningitis causes a rise in intracranial pressure [39
]. It presents in babies and in young children as a bulging or full
fontanel. In children without an open fontanel, raised intracranial pressure is
seen as other features like systemic hypertension with bradycardia. Children
may have an abnormal tone, jerky movements or be floppy
[39][40].
Other children are more likely to have the classic features of
meningitis, fever, vomiting and headache, stiff neck and photophobia.
17
Rashes may be present, most commonly when the causative
organism is Neisseria meningitidis, but more likely to be absent,
atypical, scarce or petechial in character than those seen in meningococcal
septicemia [41].
II.5.2) PARACLINICAL DIAGNOSIS OF BACTERIAL MENINGITIS
II.5.2.1) LUMBAR PUCTURE AND CSF ANALYSIS
A lumbar puncture and CSF analysis is the gold standard and
definitive diagnosis of bacterial meningitis. It is done in either sitting or
lateral decubitus position and is important to monitor the patient visually and
with a pulse oximetry for any signs of respiratory difficulties as a result of
the assumed position.
The subarachnoid space should be entered below the level of
spinal cord termination (Figure 5), and any of the interspace between L3 -L4
and L5 -S1 in children
Analysis of CSF should include: Gram stain and cultures; white
blood cell (WBC) count and differential; Glucose and protein concentrations;
Cytocentrifugation of the CSF enhancing the ability to detect bacteria and
perform a more accurate determination of the WBC differential
[23].
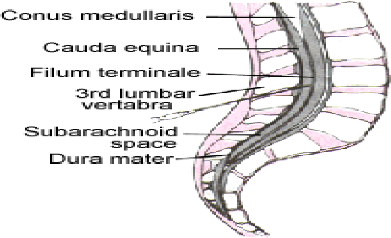
Figure 5: Lumbar spine anatomy[41].
18
Typically, the CSF white cell count (wcc) is >1000
cells/mm3 although it may not be elevated in the early phase of the infection
and the majority of white cells are polymorph nuclear (PMNs). CSF protein is
typically elevated (100-200 mg/dL) and glucose low (CSF to serum ratio <0.4)
[23]
A reduced absolute CSF concentration of glucose is as
sensitive as the CSF-to serum glucose ratio in the diagnosis of bacterial
meningitis [21]
The Gram-stained smear of CSF has a lower limit of detection
of about 105 colony-forming units/mL. Of patients with untreated bacterial
meningitis, 80% to 90% have a positive CSF Gram stain. Unless unusual
pathogens, such as anaerobes, are suspected, agar plate cultures of CSF are
preferred to liquid media [21][ 23].Pleocytosis is a typical
finding in bacterial meningitis, the WBC count usually greater than 1000
cells/mm3, and there is a predominance of polymorphornuclear leukocytes.
The lumbar puncture for the cerebro spinal analysis should be
performed once the diagnosis of meningitis is suspected and after the patient
is stabilised. However, there can be reasons to delay lumbar puncture which
include the following
+ Local site for lumbar puncture: Skin infection at site of
lumbar puncture, and
anatomical abnormality at the site of lumbar puncture
site[42]
+ Patient instability: Respiratory or cardiovascular compromise,
and continuing
seizure activity[42]
+ Suspicion of space occupying lesion [42]
+ Raised intracranial pressure[42]
+ Focal seizures[42]
+ Focal neurological signs[42]
+ Reduced conscious state of GCS less than 8 and especially if
patient is comatose[42]
+ Decerebrate or decorticate posturing[42]
+ Fixed dilated or unequal pupils[42]
+ Absent dolls eye movement[42]
+ Papilledema [42]
+ Hypertension or bradycardia[42]
+ Irregular respirations[42]
+ Anticoagulations and bleeding disorders[42]
19
| 

