II. Ecotoxicological risk assessment of hospital
wastewater : a proposed framework for raw effluents discharging Int° urban
sewer network
Evens Emmanuellr2*, Yves
Perrodinl, Gérard Kecle, Jean-Marie Blanchard2,
Paul Vermande2
1 Laboratoire des Sciences de l'Environnement,
École Nationale des Travaux Publics de l'État, Rue Maurice Audin,
69518 Vaulx-en-Velin, France
2 Laboratoire d'Analyse Environnementale des
Procédés et Systèmes Industriels, Institut National des
Sciences Appliquées de Lyon, 20 avenue Albert Einstein, 69621
Villeurbanne Cedex, France
3 Unité d'Ecotoxicologie, Ecole Nationale
Vétérinaire de Lyon, BP 83, 69280 Marcy l'Etoile, France
Keywords : Hospital wastewater,
ecotoxicological risk assessment, pharmaceuticals, disinfectants, toxicity,
Vibrio fischery, Pseudokirchnerie//a subcapitata, Daphnia magna
* Corresponding author. Tel : +(33) 4 72 04 72 89; fax:+(33) 4 72
04 77 43 E-mail address : evemml eyahoo.fr
Chapitre V Application de la méthodologie
élaborée pour l'évaluation des risques
écotoxicologiques liés aux effluents hospitaliers d'une ville
d'un pays développé tempéré
Abstract
In hospital a variety of substances are in use for medical
purposes as diagnostics and research. After application, diagnostic agents,
disinfectants and excreted non-metabolized pharmaceuticals by patients, reach
the wastewater. This form of elimination may generate risks for aquatic
organisms. The aim of this study was to present (i) the steps of an ecological
risk assessment and management framework related to hospital effluents
evacuating into wastewater treatment plant (WWTP) without preliminary
treatment; and (ii) the results of its application on wastewater from an
infectious and tropical diseases department of a hospital of a big city of the
southeast of France. The characterization of effects has been made under two
assumptions, which were related to : (a) the effects of hospital wastewater on
biological treatment process of WWTP, particularly on the community of
organisms in charge of the biological decomposition of the organic malter; (b)
the effects on aquatic organisms. COD and BOD5 have been measured
for studying global organic charge. Assessment of organo halogenated compounds
was made using AOX (halogenated organic compounds absorbable on activated
carbon) concentrations. (3) Heavy metals (arsenic, cadmium, chrome, copper,
mercury, nickel, lead and zinc) were measured. Low MPP (most probable number)
for fecal bacteria has been considered as an indirect detection of antibiotics
and disinfectants presence. For toxicity assessment, bioluminescence assay
using Vibrio fischeri photobacteria, 72-h
EC50 algae growth Pseudokirchnerie//a subcapitata
and 24-h EC50 on Daphnia magna
were used. The scenario allows to a semi-quantitative risk
characterization. It needs to be improved on some aspects, particularly those
linked: to long term toxicity assessment on target organisms (bioaccumulation
of pollutants, genotoxicity, etc.); to ecotoxicological interactions between
pharmaceuticals, disinfectants used both in diagnostics and in cleaning of
surfaces, and detergents used in cleaning of surfaces ; to the interactions
into the sewage network, between the hospital effluents and the aquatic
ecosystem.
I. Introduction
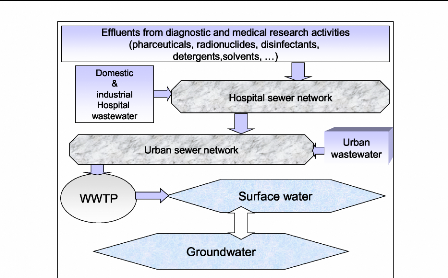
Hospitals use a variety of chemical substances such as
pharmaceuticals, radionuclides, solvents, disinfectants for medical purposes as
diagnostics, disinfections and research [1-3]. After application, some of these
substances and excreted non-metabolized drugs by the patients enter into the
hospital effluents [4, 5], which generally reach, as well as the urban
wastewater (figure 1), the municipal sewer network without preliminary
treatment [6, 7]. Unused medications also are sometimes disposed of hospital
drains [5]. Pollutants from hospital were measured in the effluents of WWTP,
and in surface water [8]. Due to laboratory and research activities or medicine
excretion into wastewater, hospitals may represent an incontestable release
source of many toxic substances in the aquatic environment [9].
Chapitre V Application de la méthodologie
élaborée pour l'évaluation des risques
écotoxicologiques liés aux effluents hospitaliers d'une ville
d'un pays développé tempéré
Hospital sewer network
V
>
/
WWTP
w
Urban wastewater
Surface water
Urban sewer network
Effluents from diagnostic and medical research activities
frskelrosesai
ri.selle. radionuclides,
elie.irdese4e1rrie.
Wi iai teGU 'Real , I ClUILMUUllUG Ul II IIGULCII IL
,
detergents,solvents, ...)
Groundwater
Domestic
&
industrial
Hospital
wastewater
Figure 1 : Problems of hospital effluents and their
impacts
on WWTP and natural environments
The contact of hospital pollutants with aquatic ecosystems
leads to a risk directly related to the existence of hazardous substances which
could have potential negative effects on biological balance of natural
environments. Risk is the probability of appearance of toxic effects after
organism exposure to hazardous substances [10]. In the context of hospital
wastewater discharge into the aquatic ecosystem, the exposure to hazardous
substances, particularly disinfectants, non-metabolized pharmaceuticals and
radionuclides, requires to consider possible risks for aquatic organisms. The
fate of pharmaceuticals in the aquatic environment have been reported in
different reviews of the literature [3, 4, 8, 11]. The ecological risk of
glutaraldehyde, a dialdehyde usually recommended as the disinfectant of choice
for reusable fiber-optic endoscopes, has been also treated in other study [9].
However, few studies treat with total risk resulting from the simultaneous
exposure to various pollutants present in the hospital effluents.
French legislation fixes the conditions for the connection of
hospital wastewater system into the urban sewer network [12]. In the Directive
N° 793/93, on the human and ecosystem exposures to the classified toxic
substances, the European Commission [13] requires to all member states to carry
out a sanitary and ecological risk assessment for substances such as: drugs,
disinfectants and radioactive substances. These regulations fall under the
context of the risk management concerning human health, and also the management
of those concerning the biological balance of the natural ecosystems. In a very
general way, the risk management always passes - formally or not - by the
preliminary phases of risk assessment [14]. The aim of this study was to
present: (i) an implemented
Chapitre V Application de la méthodologie
élaborée pour l'évaluation des risques
écotoxicologiques liés aux effluents hospitaliers d'une ville
d'un pays développé tempéré
framework for hospital wastewater management, which includes
two steps : a "light" step based on the hazard assessment related to hospital
effluents and, if proof of hazard existence occurred, the execution of a
"heavy" step, based on an ecotoxicological risk assessment of hospital
wastewater discharging into the urban sewer network, then into the natural
environment (ii) detailed elaborated procedures for the steps of "hazard
assessment" and "risk assessment" (iii) the results of their application on the
effluents of an infectious and tropical diseases department (ITDD) of a
hospital of a big city of the southeast of France.
II. Effects of hospital wastewater on aquatic
ecosystems
Hospitals consume an important volume of water per day. The
minimal domestic water consumption is 100 liters/person/day [15], whereas the
value demand for the hospitals generally varies from 400 to 1200 liters/bed/day
[16, 7]. In the United States of America, the hospital average water
consumption is 968 liters/bed/day [17]. In France, the water average needs of
university hospital centers is estimated at 750 liters/bed/day [7]. In the
developing countries, this consumption seems to be around 500 liters/bed/day
[18]. This important consumption in water of hospitals gives significant
volumes of wastewater. Results of toxicity studies using the bacteria
bioluminescence and Daphnia magna have revealed the important toxic
activities of hospital wastewater on aquatic organisms [19].
The most frequent contaminants in hospital wastewater are :
viruses and pathogenic bacteria (some of them are antibacterial resistant
characters) [20], molecules from unused and excreted nonmetabolized
pharmaceuticals [4], organohalogen compounds, such as the AOX (halogenated
organic compounds adsorbable on activated carbon) [5], radioisotopes [21,
1].
Results on the microbiological characterization of hospital
wastewater [20] reported these effluents have bacteria concentrations lower
than 108/100mL generally present in the municipal sewage system
[21]. The low most probable number (MPN) detected for fecal bacteria in
hospital is probably due to the presence of disinfectants and antibiotics [6,
20]. Markers of viral pollution of water, such as enterovirus, and other
viruses have been identified in the hospital effluents [23]. Studies on the
bacteria flora of hospital wastewater into WWTP showed that bacteria acquired
resistant character [24]. Antibacterial resistant is a threat to the efficacy
of antibacterial substances. The development of resistance to antimicrobial
agents by many bacterial pathogens has compromised traditional therapeutic
regimens, making treatment of infections more difficult [4]. Three factors have
contributed to the development and spread of resistance: mutation in common
genes that extend their spectrum of resistance, transfer of resistance genes
among diverse microorganisms, and increase in selective pressures that enhance
the development of resistant organisms [24, 25, 26, 4, 27, 28]
Hospital effluents reveal the presence of organochlorine
compounds in high concentrations [6]. AOX
up to 10 mg/L were proved in the
effluents of the hospitalization services of a university hospital
Chapitre V Application de la méthodologie
élaborée pour l'évaluation des risques
écotoxicologiques liés aux effluents hospitaliers d'une ville
d'un pays développé tempéré
center [29]. The major mass carriers for the AOX in hospital
effluents are most likely iodized X-ray contrast media, solvents,
disinfectants, cleaners and drugs containing chlorine. Brominated organic
compounds are negligible for the AOX in the hospital effluents [5]. In general,
the maximum contribution of drugs to the AOX is not above 11% [30]. Beyond that
it is also known that the AOX concentration in the urine of patients not
treated with drugs is very low. It is normally between 0.001 to 0.2 mg/L [31].
Due to the dilution effect, no substantial contribution from this source is
consequently expected [5]. The assessment of AOX shows that those non
conventional pollutants have a bad biodegradability and a bad behavior of
adsorption [8].
III. Hazard assessment
The conceptual framework for hazard assessment of hospital
wastewater (figure 2), is based on a characterization of the hospital effluents
in function: (i) of their chemical composition (measurement of global
parameters and the minerai and organic pollutants); (ii) of their
microbiological characterization; (iii) and of their intrinsic ecotoxicity.
|
|
Hospital effluents from (main or a department) collector
|
|
|
I
|
|
|
1, vl,
|
|
Chemical characterisation CC
- global parameters
- heavy metals
|
|
Microbiological characterisation MC - fecal coliforms
|
|
|
|
|
|
|
CCno regulations
|
Bioassais (UT = 100/ EC50)
- luminescence bacterial
- growth of alguae
- mobility of Daphnia
|
MC
10 NPP
|
|
Non hazardous effluents for
|
yes
|
|
yes
|
UT no
egulation
|
the ecosystems
autorisation of discharge into the urban sewer network
|
|
yes
|
|
|
Hazardous effluents for the
|
|
Hypotheses:
|
|
|
ecosystems
- presence of toxic substances
- risks for ecosystems
|
.
|
|
- presence of disinfectants,
detergents and/or surfactants - presence of antibiotics
|
|
|
|
Ecotoxicological risk assessment
|
|
|
Figure 2 : Conceptual framework for ecotoxicological
hazard
assessment of hospital wastewater
The selected parameters (stressors and assessment endpoints)
for these characterizations were: (1) COD and the BOD5 for the
measurement of the total organic load; (2) the AOX (organohalogen compounds
adsorbables on activated carbon) for the evaluation of the contained
organohalogen compounds; (3) heavy metals (arsenic, cadmium, chromium, copper,
mercury, nickel, lead and zinc) for the minerai pollution characterization; (4)
the most probable number of fecal bacteria for the microbiological
characterization (this parameter was also considered in this study like an
indirect
Chapitre V Application de la méthodologie
élaborée pour l'évaluation des risques
écotoxicologiques liés aux effluents hospitaliers d'une ville
d'un pays développé tempéré
detection of the massive presence of disinfectants and/or
antibiotics); (5) the measurement of EC50 of hospital wastewater on
bacterial luminescence (Vibrio fischen), on the algae growth
(Pseudokirchnerie//a subcapitata) and on the mobility of Daphnia
magna for the characterization of the intrinsic ecotoxicity of the
effluents.
The obtained results for these parameters have been compared
with threshold values which were established in the following way : 1) global
parameters: French regulations on effluents discharge (table 1); (2)
ecotoxicological parameters: adopted threshold values at 2 Toxic Units (UT)
[32, 19] for each of selected bioassays; (3) microbiological parameter : value
threshold fixed at 1x108 fecal coliforms for 100 ml, value
corresponding to the average content of these fecal bacteria in the
conventional urban sewer network [22].
|
Table 1: Threshold values for the different
endpoints
|
|
|
Parameters
|
Threshold values
|
Origin
|
|
Physicochemical
BOD5
COD
|
mg/L
30
125
|
[12]
[12]
|
|
AOX
|
1
|
[12]
|
|
Arsenic
|
|
|
|
Cadmium
|
|
|
|
Chromium
|
0.5
|
[12]
|
|
Copper
|
0.5
|
[12]
|
|
Mercury
|
|
|
|
Nickel
|
0.5
|
[12]
|
|
Lead
|
0.5
|
[12]
|
|
Zinc
|
2
|
[12]
|
|
Microbiological
|
|
|
|
Fecal coliforms
|
1x108
|
[22]
|
|
Bioassais
|
|
|
|
EC50 30 minutes Vibrio fischeri
|
2 UT
|
[32, 19]
|
|
EC50 72-h Pseudokirchnerie//a subcapita
|
2 UT
|
[32, 19]
|
|
EC50 48-h Daphnia magna
|
2 UT
|
[32, 19]
|
For any ratio Pc/Vt > 1 (ID,:
pollutant concentration in the hospital effluents; Vt: threshold
values) and for any number in fecal bacteria lower than 1x108 NPP
for 100mL, the framework recommends to pass at the following step : "the
ecotoxicological risk assessment of hospital wastewater".
IV. Methodological approach for the ecological risk
assessment
The ecotoxicological risk assessment is a subset of the
ecological risk assessment and can thus, for this reason, being treated
according to an approach of the same type. Ecological risk assessment is a
process that evaluates the likelihood to one or more stressors [33]. This
process is based on two major elements: characterization of effects and
characterization of exposure; these provide the focus for conducting the three
phases of risk assessment (figure 3): problem formulation, analysis phase and
risk characterization phase [34].
Chapitre V Application de la méthodologie
élaborée pour l'évaluation des risques
écotoxicologiques liés aux effluents hospitaliers d'une ville
d'un pays développé tempéré
Planning
|
|
Problem
Formulation
|
4
|
|
|
|
|
|
|
|
ul Th >.
c
Q<
|
|
Characterization
Of Of
Exposure
|
Characterization
Ecological
Effects
|
|
|
|
|
|
|
|
|
V V -
Risk characterization
|
|
Communicating results
to the risk manager
Risk management and communicating
results to interested
parties

Figure 3 : The framework for ecological risk assessment
[33]
Problem formulation
The step is a process for generating and evaluating
hypotheses about why ecological effects have occurred, or may occur, from human
activities [34]. It provides the foundation for the entire ecological risk
assessment. Problem formulation results in three products [34]: (1) assessment
endpoints that adequately reflect management goals and the ecosystem they
represent, (2) conceptual models that describe key relationships between a
stressor and assessment endpoint or between several stressors and assessment
endpoints, and (3) an analysis plan.
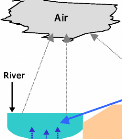
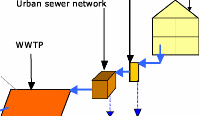
Description of the context of ecotoxicological risk
assessment
This description, whose aim was to apprehend as well
as possible the ecosystem exposure to the hospital effluents, was carried out
for a management scenario of hospital wastewater usually observed in
industrialized countries. This scenario envisages the connection of the
hospital sewer network to the urban sewer network, as well as the biological
WWTP which discharge its own effluents into the natural environment. A
synthetic description of this scenario is presented in Figure 4. The full
features ( ) indicated transport and transfers of the pollutants which has been
taken into account in the
study, whereas the features in dotted lines ( ) indicate
those which were not taken into account.
Chapitre V Application de la méthodologie
élaborée pour l'évaluation des risques
écotoxicologiques liés aux effluents hospitaliers d'une ville
d'un pays développé tempéré
Hospital sewer networ Hospital
Urban sewer network
WWTP
Unsatured zone
(semi-permeable soif)
ab Groundwater (satured zone)
·
·
·
·
·
Figure 4 : Synthetic presentation of the studied
scenario
Two types of exposed ecosystems to the hospital wastewater
pollutants have been considered in the studied scenario (table 2): (1)
artificial ecosystems represented by the WWTP and (2) natural ecosystems
represented by air, soils, surface water and groundwater.
Table 2: concerned ecosystems
Ecosystems Susceptible elements to be affected
Artificial WWTP bacteria, algae and protozoa (in case where
the biological treatment units have reactors of decomposition functioning under
the "aerobic" mode).
Air The birds and the insects
Natural Soil Microorganisms of the soils ;
Wildlife of soils (insects, earth worms,...) ;
Soil vegetables
Surface The primary producers (phytoplankton), of which
unicellular and
water pluricellular green algae ;
the primary (invertebrate), in particular of the crustaceans ;
and secondary consumers, of which fish and water birds Groundwater Protection
of fresh water resources
Development of the conceptual mode/ and choice of the
parameters of evaluation
Within the framework of this evaluation, the WWTP, the fresh
surface water and the species at the two first levels of food chains have been
considered as the targets (figure 5). The fact, that the other ecosystems and
the other species do not have been considered, does not mean that those are
less importance in the ecological level, but simply which they were not taken
into account in this first stage of the methodology development.
Chapitre V Application de la méthodologie
élaborée pour l'évaluation des risques
écotoxicologiques liés aux effluents hospitaliers d'une ville
d'un pays développé tempéré
For the characterization of the effects, two assumptions were
elaborated. They have been related to the ecological values to be protected:
(a) "the discharge of hospital pollutants into the WWTP will not affect the
biological treatment process of WWTP, with possible adverse effects on the
community of organisms in charge of the biological decomposition of the organic
malter "; (b) "the WWTP effluents will not have toxicological effects on the
living species of the natural aquatic environments".
|
Measures
|
B : bacteria (luminescence)
|
|
|
|
Effects
|
|
|
|
|
|
|
A : algae (growth)
|
|
|
|
|
|
|
|
|
|
|
C : crustacea (mobility of Daphnia)
|
Collector of hospital sewer network
{ Dilution factor : F, }
{ Dilution factor : }
{ Dilution factor : F3 }
Source Transfert
Ecosystems
Urban sewer network
Municipal WWTP
Figure 5 : Conceptuel model of the studied
scenario
The characterization of the ecological effects of hospital
pollutants on the bacteria, the algae growth and the crustacean survival, was
carried out using standardized bioassays. In this context, the bacteria were
represented by "Vibrio fischerf , the species constituting the primary
producers (phytoplankton) were represented by the algae
"Pseudokirchnerie//a subcapitata", and the fresh water crustaceans
"Daphnia magna Strauss" ensured the representation of the primary
consumers.
Analysis phase
Analysis is a process that examines the two primary components of
risk, exposure and effects, and their relationships between each other and
ecosystem characteristics [34].
Analysis phase: characterization of exposure and
ecotoxicological effects
General characteristics of studied site
Wastewater from a hospital of a big city of the southeast of
France were used for the realization of
the experimental phase of this
study. It is a hospital of 750 beds approximately. Water consumption
is
estimated at 1m3/lit/day. The effluents from the various
departments are discharged into the hospital
Chapitre V Application de la méthodologie
élaborée pour l'évaluation des risques
écotoxicologiques liés aux effluents hospitaliers d'une ville
d'un pays développé tempéré
network sewer. This network consists of several
collectors broken down by service or group of related services. The institution
has a combined sewage system. The existence of such network could increase the
concentration of the nitrogen substances during the first raining days and a
dilution of all the pollutants during the other raining days [35]. This network
could also increase the concentration of certain heavy metals, particularly
zinc.
Effluents sampling
Two campaigns of sampling (2001 and 2002) were
realized on the effluents from the infectious and tropical diseases department
(ITDD), with a capacity of 144 beds, of the hospital. Wastewater was collected
before entering into the entire hospital sewer network, which discharges the
total volume of effluents from the various departments into the urban
wastewater network without pre-treatment. This ITDD collector does not receive
effluents containing iodized X-ray contrant media from radiography department,
substances which mainly contribute to AOX formation in hospital wastewater [8].
Water samples were collected by means of a telescopic perch in a 1-L glass
flask. Ail the water samples and the mixture were kept at 4°C until
analysis.
Physicochemical analysis
pH was measured directly on site after sampling with a
pH meter HANNA instrument HI 8417 (accuracy pH #177; 0.01pH, mV #177; 0.2 mV
#177; 1, °C #177; 0.4°C) digit and standard electrode HI 1131 B
(refillable glass combination pH electrode).
Heavy metals have been determined according to ISO 11
885 protocol on filtered sample (0.45 pm) and acidified using nitric acid
(pH<2) and using ICP-AES (Inductively Coupled Plasma-Atom Emission
Spectroscopy).
Total suspended solids (TSS) concentrations were
determined in conformity with the European standard NF EN 872 after filtration
through a 1.2 pm membrane and dewatering at 105 °C.
Chlorides were determined by following the European
standard NF EN ISO 10304-1 on diluted and filtered samples at 0.45 pm by using
DIONEX DX-100 ion chromatograph with suppressed conductivity detection from 0.0
to 1000 pS. Ionpac AS14 4x250 mm analytical column (P/N 046124) was used for
chloride sample analysis. AOX were measured according to European standard EN
1485. COD concentrations in 2001 samples was measured by potassium dichromate
method using HACH spectrophotometer 2010 and test procedure provided by the
supplier. French standard NF T90-001 had been followed in the determination of
COD concentrations in 2002 samples. BOD5 concentrations in the 2001
and 2002 samples were carried out by following European and French standard NF
EN 1899-1.
Chapitre V Application de la méthodologie
élaborée pour l'évaluation des risques
écotoxicologiques liés aux effluents hospitaliers d'une ville
d'un pays développé tempéré
Total Organic Carbon (TOC) was carried out on filtered samples
at 0.45 pm and pre-treated with orthophosphoric acid (H3PO4). French
standard T90-102 was followed by using a carbon analyzer SPECTRA France, LABTOC
model, with potassium per sulfate reagent (K2S208) and UV oxidation.
Microbiological analysis
Fecal bacteria have been studied using French standard NF T
90-433 micro plaque. The French standard NF T 90-432 micro plaque and NF T
90-145 have been respectively used for the determination of faecal
streptococci and Clostridia (anaerobic spore forming bacterium).
Toxicity test procedures
For the study of assessment endpoints, three standardized
bioassays were carried out. Results of EC50 for all these bioassays,
with their confidence interval, are expressed in percentage of sample dilution
in toxic unit TU (1 TU = 100 / EC50)
·
The bioassay on bacteria luminescence was carried out with a
LUMIStox system (Dr Lange GmbH, Duesseldorf, Germany) following the standard
procedure of the European standard NF EN ISO 113483 (AFNOR, 1999). Tests were
performed using gram negative marine bioluminescent bacteria of the species
Vibrio fischeri NRRL-B-11177 of the Vibrionaceae family. In
order to prevent the interferences of TSS on the bacteria luminescence, samples
were filtered using a 0.45pm pore size membrane. The samples were treated with
NaCI solution of 20 g/L and brought to 50 mS/cm of conductivity before the
analysis. Starting from the concentration of the sample, eight consecutive
elutions were tested (dilution factor 1:2); the inhibition of bioluminescence
was measured at a wavelength of 490 nm, with readings after 5, 15 and 30
minutes of incubation at 15 °C. The EC50 values were calculated
as reported by Bulich [36].
The 72-h EC50 algae growth toxicity test was
monitored using French standard NF T90-375. Assays was carried out with the
green algae inoculums Pseudokirchnerie//a subcapitata (formerly
Selenastrum capricornutum) resulting from laboratory culture in
exponential growth phases (POLDEN of the National Institute of Applied Sciences
of Lyon -- INSA de Lyon). The sensibility of the laboratory species was
controlled by regular tests with potassium dichromate. Standard diluted medium
was used with 0.1 mg of EDTA per liter of assay solution. In order to avoid the
interferences of suspended solids and other microorganisms on algae growth
during the realization of the assay, experimental solutions were filtered at
0.45 pm. Experimental solutions were maintained at 4°C #177; 3°C. A
set of five concentrations of experimental solution samples in the reference
medium and a control were examined in each test. Assays were carried out in
glass cups containing 25 mL of samples, with 3 replicates by concentration. The
assay is static, under magnetic agitator and under constant luminosity, at
23°C #177; 2°C . Algae concentration were measured all the 24 hours
using Malassez cell and optic microscope.
Chapitre V Application de la méthodologie
élaborée pour l'évaluation des risques
écotoxicologiques liés aux effluents hospitaliers d'une ville
d'un pays développé tempéré
The determination of the inhibition of Daphnia magna
mobility is a acute toxicity assay. Its objective is to identify the
initial concentration of a pollutant in solution or an aqueous mixture which
may immobilize in 24 or 48 hours 50% of exposed daphnia into polluted
solutions. According to the European standard NF EN ISO 6341, the different
assays were carried out on Daphnia sp. maintained in parthenogenetic
culture in the laboratory (POLDEN of the National Institute of Applied Sciences
of Lyon -- INSA de Lyon). The sensibility of the laboratory species was
controlled by regular tests with potassium dichromate. Young female Daphnia,
aged less 24 h were only used. The normal medium, without EDTA, was also used.
The essays were realized at 20 #177; 2°C under darkness condition. All the
assays were carried out in a limit of time from 6 to 48 h after sampling.
Because hospital wastewater is considered as toxic for aquatic environment, a
volume of 250 mL unfiltered samples was taken for each assay. In order to
understand the effects of color, turbidity and TSS present in hospital effluent
samples on Daphnia sp., the toxicity of 250 mL filtered sample (0.45
pm pore size membrane) was studied by comparing the results with the unfiltered
volume of the same sample. The three required conditions for the validity of
assays were observed: (i) the concentration of dissolved oxygen (DO), in the
control group, was 2 mg/L at the end of each assay; (ii) the observed
percentage of immobilization in the control group vessels was 10%; (iii)
EC50 in 24h of potassium dichromate was between 0.6 to 1.7 mg/L.
Risk characterization phase
This operation is the final phase of ecological risk
assessment and is the culmination of the planning, problem formulation, and
analysis of predicted or observed adverse ecological effects related to the
assessment endpoints [34]. There is a range of possible methods, of variable
complexity [14]. The choice will depend on the operational constraints and the
available data. Rivière [10] note "the ecological risk can be expressed
of various manners: qualitative (absence or not of risk), semiquantitative
(weak, average, high risk), in probabilistic terms (the risk is x%)".
The method known as "the quotient" is the most widespread
method for the semi-quantitative characterization of risks. This method
consists in calculating the ratio (or quotient) which is expressed as a
"probable exposure concentration (PEC)" divided by a "probable non
concentration effect (PNEC)" [34]. This "probable concentration without effect"
can be estimated starting from the available data in the literature for the
pure substances, and using experimental measurements (bioassays) for the
mixture such as the hospital effluents. Although the toxicity of a chemical
mixture may be greater or less than predicted from toxicities of individual
constituents of the mixture, a quotient addition approach assumes that
toxicities are additive or approximately additive [34]. This assumption may be
most applicable when the modes of actions of chemicals in a mixture are
similar, but there is evidence that even with chemicals having dissimilar modes
of action, additive or near-additive interactions are common [37, 38, 39,
34].
Chapitre V Application de la méthodologie
élaborée pour l'évaluation des risques
écotoxicologiques liés aux effluents hospitaliers d'une ville
d'un pays développé tempéré
When the quotient value "Q" is greater than 1, the risk is
considered as significant, and all the more extremely as the quotient is large.
Conversely, more the quotient is lower than 1, more the risk is regarded as
weak. The "probable concentration without effect" on the organism is, in
practice, generally represented by a EC10, or a EC20, or a NOEC,
divided by a safety factor (10 for example). In the absence of a
EC10 or of a NOEC, the EC50 is sometimes used with a
rated-up safety factor [14].
V. Application of the step to the effluents of the
studied hospital
Resuits of the physicochemical analysis
The highest concentrations obtained for the physicochemical
characterization of the hospital wastewater from ITDD are summarized in tables
3. In all studied samples of the two campaigns (2001 and 2002), pH was always
in an alkaline range (7.7 -- 8.8) with a variation lower than 1 pH unit.
Table 3 : Physicochemical characterization of hospital
wastewater from ITDD
Parameters Units Highest concentrations
pH U
Chlorides mg/L
AOX mg/L
TSS mg/L
BOD5 mg/L
COD mg/L
TOC mg/L
TC mg/L
Heavy metals
Silver mg/L
Arsenic mg/L
Cadmium mg/L
Chromium mg/L
Copper mg/L
Mercury mg/L
Nickel mg/L
Lead mg/L
Zinc mg/L
2001
|
2002
|
|
8.8
|
8.2
|
|
359
|
127.1
|
|
1.24
|
1.61
|
|
298
|
236
|
|
1559
|
1530
|
|
2516
|
2664
|
|
350
|
3095
|
|
376
|
3183
|
|
<0,0005
|
ND
|
|
ND
|
0,011
|
|
ND
|
<0,007
|
|
ND
|
<0,004
|
|
ND
|
0,112
|
|
<0,0005
|
NM
|
|
ND
|
<0,0007
|
|
ND
|
<0,0035
|
|
ND
|
0,536
|
Microbiological characterization
Low concentrations of bacteria flora were deducted for the
hospital effluents. The results of the bacteriological characterization are
summarized in table 4.
Table 4 : Microbiological characterization of hospital
effluents from ITDD
|
Parameters
|
Units
|
Maximal concentrations
|
|
|
2001
|
2002
|
|
Fecal coliforms
|
MPN/100 mL
|
2 x 103
|
1 x 106
|
|
Fecal streptococcus
|
MPN/100 mL
|
1 x 103
|
9 x 105
|
|
Clostridia
|
UFC/20 mL
|
ND
|
104
|
Chapitre V Application de la méthodologie
élaborée pour l'évaluation des risques
écotoxicologiques liés aux effluents hospitaliers d'une ville
d'un pays développé tempéré
Ecotoxicological characterization of ITDD wastewater
The obtained results for the bioassays are synthesized in
table 5. All obtained CE50 from algae and Daphnia magna
bioassays were greater than 2 TU. The results of toxicity test on
Vibrio fischeri obtained for the year 2001, lead to EC50 (5
minutes) greater than 50% of effluent for all the samples, i.e. with an
ecotoxicity, expressed in UT, always lower than 2 UT. These results showed that
5 min assay can be considered as no toxic. However, significant differences
were observed between EC50 (5 minutes) and obtained results for
EC50 (15 and 30 minutes). In addition, there exists very little
differences between the obtained results for 15 and 30 minutes assays. This
report can be correlated with the contact time of 20 minutes contact required
by chlorinated disinfectants to inactivate bacteria [40]. The results of 15 and
30 min greater than 2 TU. The maximal concentrations ranged from 4.2 to 4.6
showed that the hospital wastewater toxicity on Vibrio fischeri are
similar to domestic wastewater toxicity. However, all the obtained results were
lower than the means of 6.75 TU reported by the literature for the toxicity of
hospital wastewater on V. fischeri completed after 30 min of exposure
[19].
Table 5 : Ecotoxicological characterizations of
hospital wastewater
Units Highest effective Variations of EC50
(2001-2002)
concentrations
(H EC50).
Parameters 2001 2002 Means Minima Maxima SD n
EC50 5 min. UT 1,54 2,5 - <1,3 2,5 9
Vibrio
fischery
EC50 15 min. UT 4,15 4,2 <1,3 4,2 9
Vibrio fischery
EC50 30 min. UT NM 4,6 <1,3 4,6 5
Vibrio fischery
EC50 72 h UT NM 56 32 9 56 18 5
Pseudokirchneri
ella subcapitata
EC50 24 h UT 117 62 43 10 117 27 13
Daphnia
EC50 48 h UT NM 71 58 52 71 9 4
Daphnia
Hazard assessment
According to the proposed framework, the hazard assessment of
hospital effluents to the aquatic ecosystems consists to compare the obtained
results for physicochemical, microbiological and ecotoxicological
characterizations with the threshold values presented in table 1 for the
different parameters. Table 6 showed the results of this comparison.
Chapitre V Application de la méthodologie
élaborée pour l'évaluation des risques
écotoxicologiques liés aux effluents hospitaliers d'une ville
d'un pays développé tempéré
Table 6 : Comparison of the highest concentrations with
the threshold values
|
Parameters
|
Units
|
Highest measured
concentrations
|
Threshold values
|
Ratio
Pc/Vt
|
|
Physicochemical
|
|
|
|
|
|
BOD5
|
mg/L
|
1559
|
30
|
>1
|
|
COD
|
mg/L
|
2664
|
125
|
>1
|
|
AOX
|
mg/L
|
1,61
|
1
|
>1
|
|
Chromium
|
mg/L
|
<0,004
|
0,5
|
<1
|
|
Copper
|
mg/L
|
0,112
|
0,5
|
<1
|
|
Nickel
|
mg/L
|
<0,0007
|
0,5
|
<1
|
|
Lead
|
mg/L
|
<0,0035
|
0,5
|
<1
|
|
Zinc
|
mg/L
|
0,536
|
2
|
<1
|
|
Microbiological
|
|
|
|
|
|
Fecal bacteria
|
NPP/100 mL
|
1 x 106
|
1x108
|
<1
|
|
Ecotoxicological
|
|
|
|
|
|
EC50 30 min. Vibrio
fischery
|
UT
|
4,6
|
2
|
>1
|
|
EC50 72 h
|
UT
|
56
|
2
|
>1
|
|
Pseudokirchnerie//a subcapitata
|
|
|
|
|
|
EC50 24 h Daphnia
|
UT
|
117
|
2
|
>1
|
|
EC50 48 h Daphnia
|
UT
|
71
|
2
|
>1
|
With the exception of the heavy metals, all the ratios
Pc/Vt carried out for the other physicochemical
parameters were greater than 1. The same observation was made for the bioassays
ratios. In addition, the results of genotoxicity tests on hospital wastewater
using AMES and HAMSTER, reported in the literature, indicated that the
effluents from clinicat services and hospital laboratories have presented a
genotoxicity character [29].
The ratio, by dividing the MPN/100 mL of fecal bacteria from
hospital wastewater with the average of those usually found in the urban
effluents, was largely lower than 1, that could, at least partially, being
related to the presence of disinfectants and/or antibiotics in the
effluents.
Ail the results confirm the existence of hazardous substances
in the studied hospital effluents, and thus the need for continuing the
approach by the setting of the ecotoxicological risk assessment of hospital
wastewater for the concerned aquatic ecosystems (WWTP and natural
environment).
Ecotoxicological risk assessment
In the absence within the hospital of pollution control
practices for wastewater, or of its own WWTP, all the contained pollutants into
the ITDD effluents as those of the whole of the hospital are evacuated towards
the municipal WWTP. In the proposed scenario, an &Oficial ecosystem "the
WWTP" as well as the natural aquatic ecosystem were retained as targets, by
restricting the study to the species of the two first levels of aquatic food
chains.
Chapitre V Application de la méthodologie
élaborée pour l'évaluation des risques
écotoxicologiques liés aux effluents hospitaliers d'une ville
d'un pays développé tempéré
Impacts on the WWTP
Assumption: " the discharge of hospital pollutants into the
WWTP will not affect the biological treatment process of WWTP, with possible
adverse effects on the community of organisms in charge of the biological
decomposition of the organic malter ".
The preservation of the biological efficiency of a WWTP can,
in a first approach, being evaluated by means of the biodegradability studies
of inflow pollutants. The biodegradability of organic substances is a measure
of the speed and completeness of its biodegradability by microorganisms [41],
and therefore the BOD5/COD ratios could be used to analyze the
difficulty or not for organic substances to be degraded [42]. A
BOD5/COD of ratio 0.5 or greater could be considered as threshold
value to study the biodegradability of organic substances into the ITDD
hospital wastewater. The variations of BOD5, COD, and the
BOD5/COD ratio in the samples of ITDD hospital wastewater, for the
2002 campaign, are showed in table 7. BOD5/DCO ratio oscillated
between 0.38 and 0.57, which indicate that the pollutants would be sometimes
difficult to degrade, which describes a potential impact on the WWTP
efficiency.
Table 7 : Variations of BOD5, COD, and
BOD5/COD ratio
|
Parameters
|
Units
|
Means
|
Minima
|
Maxima
|
SD
|
n
|
|
BOD5
|
mg/L
|
892
|
200
|
1530
|
558
|
5
|
|
COD
|
mg/L
|
1745
|
520
|
2664
|
894
|
5
|
|
BOD5/DCO
|
|
0,48
|
0,38
|
0,57
|
0,08
|
5
|
To evaluate in a semi-quantitative way the risks of a
term-source on the ecosystems in a specific context, it is possible in a first
approach, to consider the dilution coefficients generated by the global system.
Within the framework of this study, three assumptions of dilution were
considered for the risk characterization of hospital wastewater on the WWTP:
(i) the daily flow of water supply by bed per day is equal to the volume of
wastewater generated by bed per day; (ii) the ITDD generates a volume of
wastewater of 144 m3/day. In absence of specific considerations on
the interactions between the various pollutants inside the hospital sewer
network, the contained organic pollutants in the effluents of the service will
be diluted at least of 4 times in total volume, i.e. 750 m3/day of
wastewater on average are generated by the different services of the hospital,
before entering the urban sewer network; (iii) the ITDD effluents are treated
into the WWTP of the considered city, this plant receives on average a
hydraulic daily load of 87000 m3, which ensures a dilution of the
measured pollutant concentrations in the hospital effluents at least of 600
times.
In this context, the ITDD effluents will not have a significant
effect on total efficiency of the WWTP.
Indeed, if taking into account the
fact that the evaluation of WWTP efficiency is expressed as a
percentage (70
to 90 %) of degradation of the organic matters, the WWTP mechanisms will be
always
Chapitre V Application de la méthodologie
élaborée pour l'évaluation des risques
écotoxicologiques liés aux effluents hospitaliers d'une ville
d'un pays développé tempéré
able to reach this efficiency level fixed by the regulation,
since this performance at the end of process remains a function of the input
concentrations. However, this method of evaluation will not allow to prevent
the discharge into WWTP effluents of low biodegradable and toxic pollutants
(like pharmaceutical residues and AOX) for the ecosystems.
Impacts on the natural aquatic ecosystems
Assumption: "the WWTP effluents will not have toxicological
effects on the living species of the natural aquatic environments".
The ecotoxicity tests carried out for the hazard assessment
can be reused in this step, but by interpreting their results in the light of
the specific conditions of the studied scenario, in particular by taking in
account the dilution of hospital wastewater in the urban network then in the
target natural aquatic environment. It was seen previously that the dilution of
hospital effluents in WWTP was equal to 600. For this, it is necessary to add,
in the studied case, a dilution by 1000 of the WWTP effluents in the river
water bodies. That led in fineto a dilution of 6x105 of the
hospital effluents to their arrivai in the receiving receptor. On this basis,
the results of the various bioassays carried out on the effluents (table 8)
show that dilutions in the natural environment are largely sufficient to
protect itself from the studied ecotoxicity effects.
This very simplified and very operational first approach
implies however assumptions which for some are rather pessimistic and, for
others, relatively "imperfect" and being able, so to lead to an incomplete
assessment of long-term impacts of the hospital effluents on the natural
environments.
Concerning the "pessimistic" aspects, the reasoning is led as
if the pollutants in the hospital effluents were not degraded, and any
volatilization process has been occurred during their transport in the urban
sewer network, and during their passage in the WWTP. However, this
interpretation is not completely aberrant in comparison with the
characteristics of some pollutants such as the AOX, which are considered to be
non biodegradable with 90% by certain authors like Sprehe et al. [43]. If these
assumptions had led in fine to a positive evaluation of the
ecotoxicological risks, it would have been necessary to conduct a thorough
study of the concerned phenomena. In the contrary case which we are concerned,
savings of time and means (and thus "effectiveness") were carried out on these
points.
Concerning the aspects "incomplete assessment", the approach
based on standardized ecotoxicity test and the dilution of the effluents in the
natural environment implies imperfections on several levels: (1) the battery of
the selected bioassays is limited. Thus organisms such as fish, for example,
were not taken into account, (2) the long-term effects of the pollutants in
question on the ecosystems are complex and difficult to evaluate on the basis
of mono-specific simple test of ecotoxicity. Thus
Chapitre V Application de la méthodologie
élaborée pour l'évaluation des risques
écotoxicologiques liés aux effluents hospitaliers d'une ville
d'un pays développé tempéré
phenomena such as the genotoxicity of the pollutants or the
their bio-accumulation in the food chains or the sediments of the river (with
delay effect) were not treated. Field work and/or on reconstituted ecosystems
in laboratory, such as tests on microcosms [44, 45] would make it possible to
better apprehend these complex phenomena, (3) the reasoning on the basis of
dilution cannot be sufficient in term of decision for the environmental
protection. Indeed, of many other effluents are rejected into the same "target"
medium. It will be thus more judicious in the future, and for an enlightened
decision-making of the managers, to reason rather in term of contribution of
the hospital effluents to the total risk generated by the discharge of all the
industrial and urban effluents in the concerned river.
Conclusion
This study has demonstrated that it is possible to carry out
the ecotoxicological risk assessment of hospital effluents by the use of
standardized bioassays, global physicochemical parameters and the analysis of
some targeted pollutants. The proposed scenario allows to a semi-quantitative
risk characterization for the WWTP and the fresh surface water. The evaluation
will have now to be improved on certain aspects, and will require in particular
a better knowledge on the fates of pollutants in the urban sewer network and in
the WWTP. This improvement of knowledge will relate in particular to the study
of chemical and ecotoxicological interactions between pharmaceuticals,
disinfectants, and surfactants. It seems necessary to characterize the
ecotoxicological risk of the hospital effluents by experimental and fundamental
studies on the fates of disinfectants, pharmaceuticals and surfactants present
in the hospital effluents, while having care to include, on the
ecotoxicological plan, the transfers towards the food chains.
References
[1] B. Erlandsson and S. Matsson, Water, Air, and Soil Pollution
2 (1978) 199
[2] M.L. Richardson and J.M. Bowron, Pharmacol. 37 (1985) 1
[3] K. Kümmerer, M. Meyer, T. Steger-Hartmann, Wat. Res. 11
(1997) 2705
[4] B. Halling-Sorensen, N. Nielsen, P.F. Lanzky, F. Ingerslev,
H.C. Holten-Lützhoft, S.E. Jorgensen, Chemosphere 36 (1998) 357
[5] K. Kümmerer, Chemosphere 45 (2001) 957
[6] P. Leprat, Revue Techniques hospitalières 632 (1998)
49
[7] CLIN (Coordination de Luttes contre les Infections
Nosocomiales), Élimination des effluents liquides des
établissements hospitaliers -- Recommandations. Institut
Biomédical des Cordeliers, Paris, 1999, p. 74.
[8] M. Sprehe, S-U. Geipen, A. Vogelpohl, Korrespondenz
Abwasser 4 (1999) 548
[9] B. Jolibois, M. Guerber, S. Vassal, Arch. Environ.
Contam. Toxicol. 42 (2002) 137 2002
[10] J-L. Rivière, Évaluation du risque
écologique des sols pollués. Association RE.C.O.R.D., Lavoisier
Tec&Doc, Paris, 1998, p. 230.
Chapitre V Application de la méthodologie
élaborée pour l'évaluation des risques
écotoxicologiques liés aux effluents hospitaliers d'une ville
d'un pays développé tempéré
[11] T. Heberer, Toxicology Letters, 131 (2002) 5
[12] MATE (Ministère de l'aménagement du
territoire et de l'environnement), Journal Officiel de la France 52 (1998)
3247
[13] European Commission, Technical guidance document in
support of Commission Directive 93/67/EEC on risk assessment for new notified
substances and Commission Regulation (EC) n° 1488/94 on risk assessment
for existing substances, Brussels, 1995.
[14] M. Babut and Y. Perrodin, Evaluation
écotoxicologique de sédiments contaminés ou de
matériaux de dragage -- (I) Présentation & Justification de
la démarche. Cemagref -- ENTPE, Lyon, 2001, 59 p.
[15] F. Gadelle, Sécheresse 1 (1995) 11
[16] N. Deloffre-Bonnamour, Les rejets des
établissements de santé : des effluents liquides aux
déchets solides. Mémoire de Maîtrise, Université
Claude Bernard-Lyon1, Institut Universitaire Professionnalisé,
Génie de l'Environnement--Ecodéveloppement, Lyon, 1995, 75 p.
[17] U.S. EPA (United States Environmental Protection
Agency), Preliminary data summary for the hospitals point source category.
Office of water regulations and standards, Office of water, U.S. EPA,
Washington, D.C., 1989, 76 p.
[18] J. Laber, H. Raimund, R. Shrestha, Wat. Sci. Tech. 3
(1999) 317
[19] P. Jehannin, Caractérisation et gestion des
rejets liquides hospitaliers -- Etude particulière de la situation du
C.H. de Hyères (Var). Mémoire de fin d'études, Ecole
Nationale de la Santé Publique, Rennes; 1999, 71 p.
[20] S. Bernet and M. Fines, In : RRH (Réseau
Régional d'Hygiène), Actes de la Quatrième journée
du Réseau Régional d'Hygiène de Basse-Normandie, Caen,
France, 2000.
[21] J. Rodier, Bulletin de l'Association pharmaceutique
française pour l'hydrologie 4 (1971) 1
[22] Metcalf and Eddy, Wastewater Engineering: Treatment,
disposai, and reuse, 31t1 ed, McGraw-Hill, New York, 1991, 1334
p.
[23] F. Mansotte and E. Jestin, Les rejets liquides des
établissements de santé : Caractérisation à la
source et impact sur l'environnement marin côtier. Direction
Départementale des Affaires Sanitaires et Sociales de la Seine Maritime,
Agence de l'Eau de la Seine Normandie, Nanterre, 2000, 73 p.
[24] R. Thomazeau, Contribution à l'étude de
l'écologie bactérienne des boues activées. Thèse,
Université Paris VII, Paris, 1983, 250 p.
[25] A. Muela, I. Pocino, J. Arana, J. Justo, J. Iriberri, J.
Barcina, Appl. Environ. Micriobiol. 60 (1994) 4273
[26] T. Barkay, N. Kroer, L.D. Rasmussen, S. Sorensen, FEMS
Microbioly Ecolology, 16 (1995) 43
[27] J. Davison, Plasmid 42 (1999) 73
[28] T. Schwartz, W. Kohnen, B. Jansen, U. Obst, FEMS
Microbiology Ecology, 1470 (2002) 1
[29] St. Gartiser, L. Brinkler, T. Erbe, K. Kümmerer, R.
Willmund, Acta hydrochim. Hydrobio. 2 (1996) 90
[30] K. Kümmerer, St. Gartiser, T. Erbe, L. Brinkler,
Chemosphere 36 (1998) 2437
[31] S. Schulz and H.H. Hahn, gwf Wasser Abwasser 138 (1997)
109
Chapitre V Application de la méthodologie
élaborée pour l'évaluation des risques
écotoxicologiques liés aux effluents hospitaliers d'une ville
d'un pays développé tempéré
[32] J.L. Laurent, L'assainissement des
agglomérations : techniques d'épurations actuelles et
évaluations. Etude interagences n° 27. Agences l'Eau, Direction de
l'Eau, Ministère de l'aménagement du territoire et de
l'environnement. Paris, 1994, 58 p.
[33] U.S. EPA (United States Environmental Protection
Agency). Framework for ecological risk assessment. Washington, DC: Risk
Assessment Forum, U.S. Environmental Agency, 1992, 161 p.
[34] U.S. EPA (United States Environmental Protection
Agency). Guidelines for ecological risk assessment. Washington, DC: Risk
Assessment Forum, U.S. Environmental Agency, 1998, 114 p.
[35] P.L. Harremoes and F.S. Sieker Influence of
stormwater storage tanks on pollutant discharge to receiving water. In : IWA,
Symposium Sewage and refuse, liquid waste section, Proc. 9 EWPCA-ISWA,
München, Germany, 1993, pp. 95-106.
[36] A.A. Bulich, In: C.L. Markings and R.A. Kimerle
(Ed.), Aquatic toxicology, ASTM STP 667, American Society for Testing and
Materials, Philadelphia, 1979, pp 98-106.
[37] H. Künemann, Aquatic Toxicol. 19 (1981)
229
[38] J. Hermens, H. Canton, P. Jansen, R. De Jong,
Aquatic Toxicol. 5 (1984) 143
[39] S.J. Broderius, M.D. Kahl, M.D. Hoglund, Environ.
Toxicol. Chem. 9 (1995) 1591
[40] NTP (National Toxicology Program), NTP TR 392, U.S.
Dept. of Health and Human Services, National Institutes of Health, Research
Triangle Park, NC, 1992, 466 p.
[41] D.T. Sponza, Ecotoxicology and Environmental Safety
54(2003) 74
[42] M. Seiss, A. Gahr, R. Niessner, Wat. Res., 13
(2003) 242
[43] M. Sprehe, S-U. Geipen, A. Vogelpohl, Water Science
and Technology 5 (2001) 317
[44] B. Clément and C. Cadier, Ecotoxicology
5 (1998) 279
[45] Y. Perrodin, A. Gobet, L. Grelier-Volatier, V.
Canivet, J.F. Fruget, J. Gibert, C. Texier, D. Cluzeau, L. Jocteur-Monrozier,
F. Poly, Waste Management 2 (2001) 215
Chapitre VI Etude spécifique sur le devenir de
deux désinfectants largement utilisés dans les hôpitaux :
l'hypochlorite de sodium et le glutaraldehyde
| 

