cl Stabilité des PEAEP au cours du temps
d'implantation
Des résultats obtenus en psychophysique ont
montré de grosses modifications des seuils d'inconforts et dynamiques en
fonction du temps d'implantation, ce qui sous-entend une plasticité du
système auditif. Des travaux chez l'animal ont montré par les
PEAEP (Miller et al, 1995a,b) et/ou les CAP (de Sauvage et al, 1997) des
modifications électrophysiologiques au niveau des seuils d'apparition et
de l'amplitude des réponses.
Nous avons voulu étudier, les possibles modifications
des latences des PEAEP en fonction du temps chez une population de 9
implantés cochléaires Digisonic. En effet une modification des
amplitudes en fonction de l'intensité de stimulation ne ferait que
refléter l'évolution des dynamiques ; par contre des
modifications de latences sous-entendraient des modifications au niveau du
temps de conduction ainsi que du temps de traitement par le système
auditif de l'information.
Les résultats présentés figure 99
décrivent les modifications des latences des PEAEP à un an
d'intervalle. Chaque valeur représente une moyenne d'une trentaine de
PEAEP. Aucune différence statistique n'a été
trouvée pour les latences des ondes III et V. Une étude plus
rigoureuse prenant les sujets implantés cochléaires de JO
jusqu'à J600 serait peut être plus démonstrative. En tout
cas, cette pré-étude n'a pas montré de changements
très flagrants des caractéristiques des PEAEP, ce qui nous a
encouragé à développer la technique de recueil de PEAEP
avant l'implant par une stimulation extra- cochléaire.
Un couplage entre l'étude des modifications
psychophysiques (tonie/sonie) et l'étude des caractéristiques des
PEAEP semble néanmoins très prometteur.

Figure 99 : Latences des ondes III
et V des PEAEP et durée d'implantation chez 9
sujets implantés.
dl Faisabilité en
préimplantation
L'utilisation des PEAEP avant l'implantation paraît aussi
intéressante celà soulève des problèmes
supplémentaires. La mise place d'une technique et d'un
protocole adapté semble nécessaire.
Article 16 :
ELECTRICALLY AUDITORY BRAINSTEM RESPONSES IN COCHLEAR
IMPLANT ASSESSMENT :
POSSIBILITY AND INTEREST
S. Gallégo, E. Truy, C Berger Vachon, L.
Collet
Article soumis
L'étude consiste à étudier la
faisabilité du recueil de potentiels évoqués auditifs
électriques précoces (PEAEP) avec une électrode temporaire
de stimulation. Dans un premier temps l'étude de la littérature a
permis de confirmer la faisabilité physiologique et technique des PEAEP
lors d'une stimulation électrique de la fenêtre ronde ou du
promontoire. Il a ainsi été possible de définir un
protocole d'enregistrement des PEAEP (position des électrodes de
stimulation et de recueil, paramètres d'acquisition, traitement
numérique post-acquisition). Pour finir, des résultats
préliminaires sur 9 cas ont été décrits.
L'optimisation de la technique a permis d'obtenir des PEAEP dans 78 % des
cas.
Malgré les contraintes techniques et physiologiques,
les PEAEP peuvent être enregistrés avec une électrode
temporaire sur la fenêtre ronde. Le positionnement, le choix des
électrodes de recueil et de stimulation ainsi que le traitement
numérique post-acquisition sont très important pour obtenir des
PEAEP pré-implantation. Cette technique ne peut être actuellement
que consultative car elle n'est fiable que dans 78 % des cas. Les
résultats obtenus nous encouragent cependant à la
développer et à l'étendre à une stimulation du
promontoire au lieu de la fenêtre ronde. L'enjeu est en effet important,
l'utilisation de cette méthode donnerait des éléments
objectifs qui appuieraient une décision d'implantation, aideraient
à choisir le côté à implanter et permettraient de
faire une estimation des performances du sujet après l'implantation.
ELECTRICALLY AUDITORY BRAINSTEM RESPONSES IN COCHLEAR
IMPLANT
ASSESSMENT : POSSIBILITY AND INTEREST.
S. Gallégo, E. Truy, C. Berger-Vachon, L.
Collet
UPRESA- CNRS 5020 & MXM laboratory
ABSTRACT : The present study is the
feasibility of recording electrically auditory brainstem responses (EABR) with
a temporary stimulating electrode. Preliminary study of the literature
confirmed the physiological and technical feasibility of EABR with
electro-stimulation of the round window or of the promontorium. This enabled a
EABR recording design to be drawn up: stimulating and recording electrode
positions, recording parameters and post-recording and data processing.
Finally, preliminary results for 9 cases are described. Optimising the
technique enabled EABRs to be recorded in 78 % of cases.
Key words: EABR, prior implantation test,
Cochlear Implant. INTRODUCTION
Developments in signal processing and encoding strategy for
the various cochlear implant (CI) now enable very good clinical results to be
obtained. The percentage of `star patients' (able to communicate by telephone
using only auditory information) is steadily growing. Even so, Cl subject
performances remain variable and are not totally predictable or accounted
for.
It is generally accepted that Cl bearers' pre-implantation
performance can be assessed in terms of parameters such as length of sensory
deprivation, aetiology of defect, language level, lip-reading performance,
psycho-physical performance, IQ, motivation, family back ground, ... Measuring
auditory remains (neurone population) is also a key-factor for Cl prognosis.
There at present few tests of auditory system functioning. Lusted et al (1984),
Shannon (1983) and Pfingst et al (1980, 1984) have shown threshold and comfort
levels and dynamics in implanted subjects to be closely dependent upon
aetiology and spiral ganglion neurone population.
The commonest means of assessing the remaining neurone
population is by measuring threshold and comfort levels using electrical
stimulation of the round window or of the promontorium by a temporary electrode
(House et al, 1976; Shipp et al, 1991). This test is, however, unreliable and
open to criticism, in that only positive results can be validated. Response
failure or defective levels are not necessarily indicative of an auditory
system defect, but could simply be due to faulty stimulation electrode
positioning or poor electrical diffusion in the physiological environment of
the cochlea. Moreover, the test is hard to conduct in children or in poorly
conditioned adult subjects, requiring as it does considerable patient
participation.
Error in predicting Cl performance are partly due to the lack
of objective measurements of the state of the auditory system.
Electrophysiology (i.e., evoked potentials could provide a means of
objectifying measurement so as to better quantify neurone population and the
functional state of the auditory system.
The present study used electrical stimulation of the cochlea
by a temporary electrode on the promontorium or the round window to study the
technical and physiological feasibility and the usefulness of pre-implantation
EABR recording.
Interest of pre-implantation EABR recording
There are several studies in the literature which wouid
encourage the idea of using pre-implantation EABRs as a means of predicting
post-implantation performance. Certain authors (Wesber and Wesber, 1979;
Chouard et al, 1983) have reported correlation between duration of deafness and
auditory system neurone population. Acoustic stimulation studies (Otte et al,
1978; Schmidt et al, 1985) have correlated deaf subjects' hearing loss to
spiral ganglion cell number. Pauler et al (1986) found a correlation between
intelligibility and spiral ganglion neurone population. Measuring auditory
system neurone density wouid thus allow an estimation of performance.
Studies in animais (Hall et al, 1990) and in humans (Smith et
al, 1983; Brighwell et al, 1985) have shown correlation between spiral ganglion
neurone population and ABR amplitude under electrical stimulation (EABR). Other
authors (Gallégo et al, 1997) have correlated recognition without
lip-reading in Cl-bearers to certain EABR parameters (wave Ill and V latency
interval). EABR thus do enable estimation of auditory system neurone population
and Cl-bearers' performance..
Systematic pre-implantation EABR recording would thus enable
measurement of auditory system functionaiity, estimation of its neurone
population, and prediction of performance with Cl. This could heip in decision
to implant, choice of implant-side, type of implant (mono- or multi-channel)
and of implant encoding strategy (slow or fast stimulation).
Physiological and technical constraints
Electrical stimulation to the base of the cochlea through an
extra-cochlear temporary electrode can produce auditory sensations. The
stimulating electrode may be placed either on the promontorium or on the round
window, and the techniques in the two cases are not the same. For positioning
on the promontorium , a transtympanic electrode is slipped through, without any
need of anaesthetic. Round window positioning requires lifting the tympanum and
a local anaesthetic. According to the literature (Shipp et al, 1991),
perceptual threshold measurements and test reliability are better with a round
window design; ciinical and ethical problems, however, arise, given the need
for surgery and local anaesthesia. EABR recording using a promontory
stimulating electrode has the advantage of being less invasive, even if
technically less simple to make (the electric currents are weaker and better
focussed on the cochlea with round-window stimulation). Developing EABR
recording techniques using a temporary stimulating electrode therefore needs to
start off from round-window stimulation to end up if possible with promontorium
design.
Does electrical stimulation of the base of the cochlea
generate EABR?
EABRs can be recorded from ail the Cl electrode, even the
most basal (Gallégo et al, 1996, 1997). Thus very basal stimulation can
indeed generate EABRs (even if the number of cochiear neurones thus excited is
less than for more apical stimulation). This increases the difficulty of
recording, by increasing adaptation (the smaller the number of excited neurones
the greater their adaptation) and decreasing the signalto-noise ratio). With
Cl, EABR intensity is always below comfort level threshold (Abbas and Brown,
1988; Shallop et al, 1991; Gallégo et al, 1997), which makes recording
possible without anaesthetic.
Extracochlear evoked responses
With temporary electrodes, electrical stimulates diffuses
widely in the tissue. Nonauditory responses can thus easily overlay EABRs.
Fifer et al (1990) have described myogenic responses, producing fairly high
amplitude waves with 5-7 ms latency, which badly disturb EABR recording,
masking as they do wave V.
Gyo et al (1980) and Honert and Stypulkowski (1986) have also
demonstrated the possibility of vestibular responses during the first
milliseconds, although the latencies and amplitudes of these waves in human
have not been accurately determined. Electrical stimulation can further
activate the facial and buco-pharyngeal nerves, disturbing recording by
saturating the entry amplifier of the acquisition system.
Subjects
Nine subjects took part in the present study (2 children, 7
adults). All had presented for conventional pre-implantation electrical
testing. AIl had profound or total bilateral deafness. Testing took place
without anaesthetic for 5 of adults and under general anaesthetic for 4
subjects (2 children, 2 adults).
TECHNICAL SET-UP
Positioning of stimulating and recording
electrodes
To limit stimulus artefact, electrical diffusion in the
physiological environment needs to be kept to a minimum. One way doing this is
to localise stimulation by bringing the two stimulating electrodes as close as
possible (the positive on the round window, the negative behind the ear on the
petrosal). To limit extracochlear stimulation (myogenic, vestibular,
buco-pharyngeal and facial nerve), the positive electrode is small, to focus on
the cochlea, and the negative one large, to diffuse the current outside the
cochlea, reducing charge per area. The current thus flows horizontally. To
reduce stimulus artefact, recording electrodes are placed perpendicularly to
the current flowline: positive on the forehead, negative on the chin (see fig.
1). The earth is placed on the contralateral earlobe.
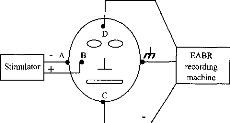
Figure 1: Synopsis of stimulating and
recording electrode positions. The axis formed by the stimulating electrodes
was perpendicular to that formed by the recording electrodes (AB perpendicular
to CD). The stimulation axis (AB) projects across the middle of the recording
segment (CD).
I deally, if the distances between the stimulus and the
positive and negative
recording electrodes are equivalent (AD=AC), and if
the angle between the recording
and the stimulating electrodes is 90°, then the stimulus
artefact cancels out in the recording.
Stimulator
The electrical stimulator was a prototype (Digistim+ system)
developed by the MXM company, which can send two phase pulsed stimulation
controlled for current, pulse duration and frequency, and can synchronise the
EABR recording system.
Recording parameters
The system recorded EABRs over 10 ms at a sampling frequency
of 50 kHz. Fullscale sensitivity was +1- 50 iiV. The analogic input filter was
0.2-8,000 Hz. Each recording corresponded to an averaging of 512 sweeps, was
safeguarded then transferred onto a PC for post-recording digital analysis.
Post-recording digital analysis
Post-recording digital filtering is a good way of enhancing
EABR curves, although conventional post-recording digital filters do not work
well as they also filter stimulus artefact effects. The digital filter used
here is specially adapted to auditory system functioning and electrical
stimulation requirements (Gallégo et al, submitted). The frequencies in
each wave have been shown to grow lower as wave latency lengthens. The idea of
the filter is to vary the transfer function according to the latency.
Simulations have shown this digital filtering to be able to reveal a EABR with
a signal-to-noise ratio of --36dB (noise some 60-foid stronger than signal);
hence it can also reduce non-auditory waves and stimulus artefact
derivatives.
Results and discussion
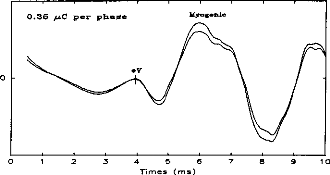
Figure 2 shows a typical case, with the EABR overlain by a
myogenic response. The wave V amplitude (around 4 ms) was much lower than the
myogenic wave's (around 6 ms). In this case, a needle electrode had been used
as negative stimulating electrode: focussing the current between the round
window and petrosal bone, it encouraged extracochlear myogenic stimulation.
o
9 10
Figure 2: Example of EABR with a myogenic
response. Wave V latency is 4.05 ms. Myogenic wave
latency is around 6 10
ms.
Figure 3 gives an example of EABRs recorded from a
non-anaesthetised adult
subject when electrode positions and recording
parameters have been optimised.
Waves III and V are easily identifiable. The
EABR wave forms and latencies are very
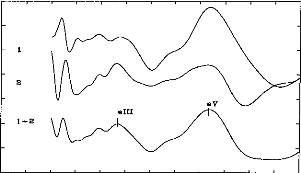
similar to those found after implantation. 1.0
0.5
0.0
>
-0.5
N
-"C:7 = :'-'
-1.0
Q
E
< -L5
- 2.0
- 2.5 0 0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0 5.5 5
0
Latence (ms)
Figure 3: Example of EABR on non-anaesthetised
subject. Wave V Iatency is 4.15 ms. Wave III Iatency is 2.35 ms.
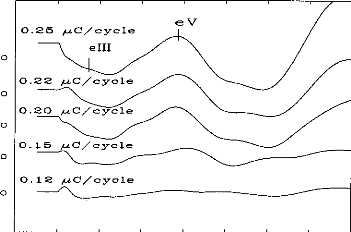
Figure 4 is an example of EABRs from a child subject under
general anaesthetic just before implantation. Wave V is easily identifiable,
but not wave III.
0 1 2 3 4 5 6 7 8
Ti me (ms)
Figure 4: Example of threshold of EABR on
general anaesthetised child. Wave V Iatency is 4.00 ms.
Out of 9 subjects tested, EABRs were obtained in only 7 cases
(78 % success rate).
Wave was aiways identifiable, but wave III only in 4
cases. Mean of wave V Iatency is
4.15 ms (S.D = 0.30 ms). Mean of wave V Iatency is 2.25 ms (S.D =
0.25 ms). Resuits are approximately the same of Cochlear Implant
(Gallégo et al, 1996, 1997).
CONCLUSION
Despite technical and physiological constraints, EABRs can be
recorded with a temporary electrode on the round window. Positioning and choice
of recording and stimulating electrodes, and post-recording digital processing,
are all very important in obtaining pre-implantation EABRs. The technique, with
only 78% reliability, is as yet of only consultative value, but the results
here nevertheless encourage development and its extension to promontory rather
than round window stimulation. The stake is high: being able to use this method
would give objective support to indications for implantation, help choose the
implant side and enable estimation of subject's' post- implantation
performance.
REFERENCES
Abbas PJ, Brown CJ. Electrically evoked brainstem potentials
in cochlear implant patients with multi-electrode stimulation. Hear Res 1988;
36:153-62.
Brightwell A, Rothera M, Conway M, Graham J. Evaluation of
status of the auditory nerve: psychophysical test and ABR. Eds RA Schindler
& MM Merzenich Cochlear Implants Raven Press New York 1985 343-349.
Chouard CH, Josset P, Meyer B, Buche JF. Effect of chronic
electrical stimulation of the auditory nerve on development of cochlear nuclei
in guinea-pig. Ann OtolLaryngol (Paris) 1983; 100:417-422.
Clark G, Shepherd R, Franz B, Dowell R, Tong Y et al. The
histopathology of the human temporary bone and auditory central nervous system
following cochlear implantation in patient. Acta Otolaryngol (Stockh) 1988;
(suppl 448):1-65.
Fifer RC, Novak MA. Myogenic Influences on the Electrical
Auditory Brainstem Response (EABR) in Humans. Laryngoscope 1990;
100:1180-1184.
Gallégo S, Micheyl C, Berger-Vachon C, Truy E, Morgon A,
Collet L. Ipsilateral ABR with cochlear implant. Acta Otolaryngol (Stockh)
1996; 116:228-233.
Gallégo S, Truy E, Morgon A, Collet L. EABRs and
surface potentials with a transcutaneous multielectrode cochlear implant. Acta
Otolaryngol (Stockh) 1997; 117:164-168.
Gallégo S, Durrant J, Collet L., Berger-Vachon C.
Numeric time-variant filters adapted to the recording of electrically auditory
brainstem responses (E-ABR). Submitted.
Gyo K, Yanagihara N. Electrically and acoustically evoked
brainstem responses in guinea pig. Acta Otolaryngol (Stockh) 1980; 90:25-31.
Hall RD. Estimation of surviving spiral ganglion cells in the
deaf rat using the
electrically evoked auditory brainstem response. Hear Res 1990;
45:123-36.
Honert van den C, Stypulkowski PH.
Characterization of the electrically evoked auditory brainstem
response (ABR) in cats and humans. Hear Res 1986; 21:109-26. House WF, Berliner
K, Crary W, Graham M, Luckey R, Norton N, Selters W, Tobin H, Urban J, Wexler
M. Cochlear implants. An Otol Rhinol Laryngol 1976; 85(suppl 27):193
Lusted H, Shelton C, Simmons S. Comparison of electrode sites in
electrical stimulation of the cochlea. Laryngoscope 1984; 94:878-882.
Miller CA, Abbas PJ, Brown CJ. Electrically evoked auditory
brainstem response to stimulation of different sites in the cochlea. Hear Res
1993 66;130-142.
Pauler M, Schuknecht H, Thornton R. Correlative studies of
cochlear neuronal loss with speech discrimination and pure-tone thresholds.
Arch Otorhinolaryngol 1986; 243:200-206.
Pfingst B, Telman S, Sutton D. Operating ranges for cochlear
implants. Ann Otol Rhinol Laryngol 1980; 89(sup 66):1-4.
Pfingst B. Operating ranges and intensity psychophysics for
cochlear implants. Arch Otolaryngol 1984; 110:140-144.
Scmidt J. Cochlear neuronal populations in developmental defects
of the inner ear: implications for cochlear implantation. Acta Otolaryngol
(Stockh) 1985; 99:14-20. Shailop JK, VanDyke L, Goin DW, Mischke RE. Prediction
of behavioral threshold and confort values for Nucleus 22-channel implant
patients from electrical auditory brain stem response test results. Ann Otol
Rhinol Laryngol 1991; 100:896-898. Shannon RV. Multichannel electrical
stimulation of the auditory nerve in man.l. Basic psychophysics. Hear Res 1983;
11:157-189.
Smith L, Simmons FB. Estimating eighth nerve survival by
electrical stimulation. Ann Otol Rhinol Laryngol 1983; 92:19-23.
Shipp DB, Nedzelski JM. Round window versus promontory
stimulation: assessment fo cochlear implant candidacy. Ann Otol Rhinol Laryngol
1991; 100:889-892. Webster DB, Webster M. Effect of neonatal conductive hearing
loss on brain stem nuclei. Ann Otol Rhinol Laryngol 1979; 88:684.
D'autres expériences, faites en collaboration avec
l'hôpital Troussaud (Messieurs les docteurs Garabédian et
Serfati), utilisant le même protocole ont permis d'obtenir des PEAEP sur
13/15 (soit 87%) des enfants testés avec une stimulation
électrique du promontoire par une électrode transtympanique. La
figure 100 illustre un des meilleurs cas.
0.211V
Figure 100 : PEAEP avec une
stimulation au promontoire chez un sujet enfant sourd sous
anesthésie
générale (avec l'aimable collaboration de
l'équipe de Mr Garabédian)
| 

