CHAPTER III: MATERIALS AND
METHOD
1. STUDY DESIGN
This was a cross-sectional analytic study.
2. DESCRIPTION OF THE STUDY SITE
This study was conducted at the external consultation service
of the cardiology unit of the Yaounde General Hospital (YGH) which is located
in Yaounde, the capital city of Cameroon.YGH serves as a teaching centre, and
is a reference hospital for other hospitals in the Centre region.
YGH is a state-owned hospital made up of several units:
internal medicine, surgery,
obstetrics, gynaecology and paediatrics. It covers an area of
20,301 square metres and as of 2001 had 302 beds. Inhabitants from Yaounde and
beyond come to this reference health institution to seek for general and
specialized health services.
3. STUDY PERIOD
This study was carried out over a period of seven months
(November 2017 - May 2018).
4. SAMPLING
4.1 Study population
Hypertensive patients receivingantihypertensive treatment as
outpatients at the YGH.
4.2 Inclusion criteria
Ø Hypertensive patients aged 18 years and above;
Ø Outpatients diagnosed with HBP and on
antihypertensive drug treatment for at least 6 months prior to recruitment
period;
Ø Patients who consent to be enrolled in the study.
4.3 Non-inclusion criteria
Outpatients with hypertension:
Ø andwith mental impairment or psychiatric disease;
Ø with difficulty in communication and without a
translator;
Ø who gave incomplete information necessary for the
study;
Ø unable or unwilling to give informed consent.
4.4 Sample size
Cochran'sformula[112],   , was used to estimatethe sample size. , was used to estimatethe sample size.
The following assumptions were made:previous data indicated an
adherence rate of 12.9% in Garoua[16]. So proportion was taken
as 12.9%(p = 0.129), 95% confidence interval, and 5% margin of error(d = 0.05).
Computing into the above formula:

n = Minimum sample size required
p= Antihypertensive adherence rate
d= Error margin of 5%
Z1-á/22 =95%
confidence interval (value type=1.96)
Therefore, from the above formula a minimum sample size of 173
patients was required for the study.
5. MATERIALS
5.1 Materials for data collection
Ø Patientmedical records.
Ø Case report forms (CRFs) for data collection.
Ø Ballpoint ink-pens, pencils, and erasers.
5.2 Materials for data analysis
Ø A laptop with Microsoft®Office Tools
2013 for data entry and Epi-infoTMsoftware Version 3.5.4 for data
analysis.
Ø An 8 GB flash disk.
5.3 Materials for Blood Pressure
Measurement
Ø A calibrated electronic sphygmomanometer (Model:
LD-578)
Ø A stethoscope
6. DATA COLLECTION PROCEDURE
Administrative and ethical approvals
In accordance with research ethics, ethical clearance was
obtained from the Institutional Review Board of the Faculty of Medicine and
Biomedical Sciences of the University of Yaounde I(APPENDIX
1A), as well as authorization from the Director of the YGH before the
recruitment of patients for the study (APPENDIX 1B). The study
was explained to the patients and informed consent by signature was obtained
prior to their enrolment into the study (APPENDIX 2). During
the study, the case report forms (APPENDIX 3) were kept secret
by the investigator from people not involved in the study, in order to respect
patient confidentiality.
Approach with the participants
The patients admitted into this study were selected
consecutively at the external consultation service of the cardiology unit.
Patients that met our inclusion criteria were selected during consultations and
interviewed immediately after. After obtaining their written consent, we
proceeded by measuring their resting BP. Two sitting BP measurements were taken
on both arms with a pretested electronic sphygmomanometer approximately 2
minutes apart. Another 2 minutes later, a third measurement was taken on the
arm with the highest BP reading. Then an average of the last two readings was
eventually used to determine the BP level during the visit. After recording the
BP reading, we proceeded with an interview of the patients in order to fill the
pretested questionnaires. BP measurements and interview were carried out in
private in a consultation box. The 2014 Evidence-Based Guideline for the
Management of High Blood Pressure in Adults[113] was used to
evaluate the level of control of patient BP:
v Hypertensive patients aged 60 years and above were
considered to have a controlled hypertension if their average BP reading
was<150/90 mmHgduring the last 3 months and if they presented with no
diabetes nor chronic kidney disease.
v Hypertensive patients aged 60 years and above were equally
considered to have a controlled hypertension if their average BP reading
was<140/90 mmHg during the last 3 monthsif they presented with diabetes or
chronic kidney disease.
v Also, patients aged under 60 were considered to have a
controlled hypertension if their average BP reading was<140/90 mmHgduring
the last 3 months and if they presented with or without other comorbidities
(diabetes and chronic kidney disease).
At the end, the questionnaires were cautiously stored prior to
data analysis.
The variables to be investigated consisted of:
Ø Sociodemographic data (independent
variables): Age, sex, zone of residence, marital status, trip duration
to the hospital, level of education, and profession.
Ø Socioeconomic data (independent
variables):Socioeconomic status (which is an adapted classification
from theRevised Kuppuswamy's socio-economic status scale- January
2015[114](see APPENDIX 3) where the projected
family income was estimated from the Gross National Income (GNI) per capital;
health insurance; monthly drug costs. A score of <5 was considered low;
between 5 and 10 was considered middle; and >10 was considered high
socioeconomic status.
Ø Clinical characteristics of
respondents(independent variables):Comorbidities present (if any);
blood pressure readings; handicap present (if any).
Classification of BP:SBP <120mmHg and DBP
<80mmHg was considered optimal; SBP [120-129]mmHg and/or DBP [80-84]mmHg was
considered normal; SBP [130-139]mmHg and/or DBP [85-89]mmHg was considered High
Normal; SBP [140-159]mmHg and/or DBP [90-99]mmHg was considered Grade I
hypertension; SBP [160-179]mmHg and/or DBP [100-109]mmHg was considered Grade
II hypertension; SBP=180mmHg and/or DBP =110mmHg was considered Grade III
hypertension; SBP =140mmHg and DBP <90mmHg was considered isolated systolic
hypertension.
Definition of heart failure:Inability of the
heart to ensure blood flow necessary for the metabolic and functional needs of
body organs. Clinical signs include edema, tachycardia, and rales with low
ejection fraction (EF<43%).
Diagnostic criteria for
hypercholesterolemia:
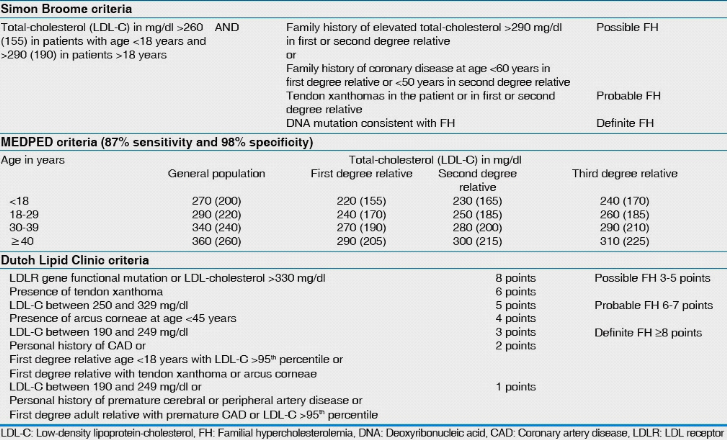
Figure 7: Dutch Lipid
Clinic criteria
Definition of obesity:BMI >24.9
kg/m2.
Diagnostic criteria for diabetes: A1C =6.5%
or Fasting Plasma Glucose =126 mg/dl (7.0 mmol/l) or 2-h plasma glucose =200
mg/dl (11.1 mmol/l) during an Oral Glucose Tolerance Test or in a patient with
classic symptoms of hyperglycemia or hyperglycemic crisis, a random plasma
glucose =200 mg/dl (11.1 mmol/l).
Definition of gout:Inflammatory
microcrystalline arthropathy associated with intense pain and related to a
disruption of the metabolism ofuric acid.Hyperuricemia is generally above 390
umol/L (6.5 mg/dL).
Diagnostic criteria for arthritis:Prolonged
morning stiffness, swollen joints, and painful/inflamed joints.
Diagnostic criteria for gastritis: Nausea,
abdominal pain, bloating, vomiting, indigestion, and burning feeling in the
epigastric region.
Diagnostic criteria for hyperthyroidism:
Nervousness, mood swings, muscle weakness, heat intolerance, insomnia,
hand tremors, tachycardia, diarrhea, weight loss, enlarged thyroid gland, and
elevated thyroid stimulating hormone, free thyroxine and total triiodothyronine
levels.
Definition of epilepsy: Presence or history
of recurrent convulsions which are involuntary, violent, and spasmodic or
prolonged contraction of skeletal muscles.
Definition of anemia: Decrease in hemoglobin
per unit of blood volume below physiological values i.e. 13 g / dL in men; 12 g
/ dL in women and children.
Diagnostic criteria for benign prostate
hypertrophy: Presence of enlarged prostate, high prostate specific
antigen levels, polyuria, weak stream and/or urinary incontinence.
Diagnostic criteria for depression: Presence
of psychological symptoms (low mood, low self-esteem, feeling irritable, no
interest in things, anxiety, suicidal thoughts); and physical symptoms (changes
in weight, constipation, unexplained pains, loss of libido, changes in
menstrual cycle).
Definition of glaucoma: Intraocular pressure
above an upper normal value of 21 mmHg.
Diagnostic criteria for hemorrhoids: Presence
of bleeding with or without defecation, mucous discharge, pruritus, incomplete
evacuation, distal rectal mass upon digital exam, and presence of fissures
after anoscopy.
Diagnostic criteria for deep venous thrombosis:
Presence of pain, swelling and tenderness in legs, warm skin in the
area of the clot upon palpation, positive D-dimer test, detection of clots with
Doppler ultrasound.
Definition of physical handicap: Presence of
physical defects, including upper or lower limb loss or poor manual
dexterity.
Definition of sensory handicap: Presence of
visual impairment or blindness, hearing loss or deafness.
Ø Therapeutic characteristics of
respondents(independent variables): Type of therapy; molecule(s)
prescribed;Drugs prescribed (pioneer or generic); Antihypertensive drug groups
prescribed; number of drugs used per day; Dosage schedule; Presence of side
effects (if any); Duration onantihypertensive treatment.
Ø Adherence profile (dependent
variable):The Eight-Item Medication Adherence Scale (Table VI) was
used to assess therapeutic adherence[95].
We assessed the adherence level of the study population by
using the validated MMAS-8. The scale is based on patients`
self-response.Patients with a score of 8 on the scale were termed highly
adherent, medium adherers were those with a score of 6 to <8, and those
classified as lowadherers were those with a score of <6.This medication
adherence scale has the advantage of beingrelatively simple and practical to
use in clinical settings. The instrument was used to identify patients with
adherence problems, and could also be used to monitor adherence over the course
of the treatment. One important feature of the scale is that treatment-related
attitudinal and behavioral problems thatthe patient may be facing can be
immediately identified and health care providers may provide reinforcement and
advice such that the patient can take positive steps early on to address these
issues. Patients were considered to have a poor adherence if they had <8 and
good adherence if they scored 8 on the MMAS-8 (Table VII).
Ø Patient knowledge (independent
variable)
Data concerning patients' knowledge of hypertension (i.e.
causes, treatment, and complications) was also collected on the pretested
questionnaires (APPENDIX 3). Knowledge scores for individuals
were calculated and summed up to give a total knowledge score. The scoring
range isfrom 0 (minimum) to 16 (maximum). A cut-off score of <8 was
considered as poor knowledge, ascore of [8-12] was considered knowledgeable and
a score of [13-16] was considered good knowledge.
Table VI: The 8-Item Medication Adherence
Scale[95]
|
ITEM
|
CORRECTED ITEM-TO-TOTAL CORRELATION
|
|
1. Do you sometimes forget to take your
high blood pressure
pills?
|
.4639
|
|
2. Over the past 2 weeks, were there any
days when you did
not take your high
blood pressure medicine?
|
.5108
|
|
3. Have you ever cut back or stopped
taking your medication
without telling
your doctor because you felt worse
when you took it?
|
.4277
|
|
4. When you travel or leave home, do you
sometimes forget
to bring along your
medications?
|
.4095
|
|
5. Did you take your high blood pressure
medicine
yesterday?
|
.3038
|
|
6. When you feel like your blood pressure
is under control,
do you sometimes
stop taking your medicine?
|
.5044
|
|
7. Taking medication everyday is a real
inconvenience for
some people. Do you
ever feel hassled about sticking to your
blood
pressure treatment plan?
|
.4009
|
|
8. How often do you have difficulty
remembering to take all
your blood
pressure medication?
|
.5896
|
|
á Reliability, .83.
|
|
Table VII: Cut-offs for
MMAS-8
|
Cut-off score
|
Adherence status
|
|
8
|
High adherers
|
Good adherence
|
|
|
|
|
[6-8[
|
Medium adherers
|
Poor adherence
|
|
<6
|
Low adherers
|
7. STATISTICAL ANALYSIS
Data entry and analysis was undertaken using the statistical
software Epi Info version 3.5.4. Data cleaning was performed to check for
accuracy, consistency and that there were no missed values during entry.
Frequencies, proportions and summary statistics were equally generated to
describe the study population in relation to the relevant variables.Bivariate
analysis using the chi2test was carried out to assess associations of each
independent variable with thedependent variable. Variables with P-value<
0.05 in bivariate analysis were selected as candidate variables for
multivariate analysis with logistic regression. Odds ratio and 95% confidence
interval were used to identify the presence andstrength of association.
Statistical significance was considered at P-value < 0.05.
8. HUMAN RESOURCES
Ø Supervisor: Pr MENANGA Alain Patrick
Ø Co-supervisor: Dr. TEMBE Estella épse FOKUNANG
Ø Investigator: CHIABI Roland MUNTOH
Ø Collaborators: Medical and paramedical personnel
Ø A statistician
| 

